Management of Breech Presentation (Green-top Guideline No. 20b)
Summary: The aim of this guideline is to aid decision making regarding the route of delivery and choice of various techniques used during delivery. It does not include antenatal or postnatal care. Information regarding external cephalic version is the topic of the separate Royal College of Obstetricians and Gynaecologists Green-top Guideline No. 20a, External Cephalic Version and Reducing the Incidence of Term Breech Presentation .
Breech presentation occurs in 3–4% of term deliveries and is more common in preterm deliveries and nulliparous women. Breech presentation is associated with uterine and congenital abnormalities, and has a significant recurrence risk. Term babies presenting by the breech have worse outcomes than cephalic presenting babies, irrespective of the mode of delivery.
A large reduction in the incidence of planned vaginal breech birth followed publication of the Term Breech Trial. Nevertheless, due to various circumstances vaginal breech births will continue. Lack of experience has led to a loss of skills essential for these deliveries. Conversely, caesarean section can has serious long-term consequences.
COVID disclaimer: This guideline was developed as part of the regular updates to programme of Green-top Guidelines, as outlined in our document Developing a Green-top Guideline: Guidance for developers , and prior to the emergence of COVID-19.
Version history: This is the fourth edition of this guideline.
Please note that the RCOG Guidelines Committee regularly assesses the need to update the information provided in this publication. Further information on this review is available on request.
Developer declaration of interests:
Mr M Griffiths is a member of Doctors for a Woman's right to Choose on Abortion. He is an unpaid member of a Quality Standards Advisory Committee at NICE, for which he does receive expenses for related travel, accommodation and meals.
Mr LWM Impey is Director of Oxford Fetal Medicine Ltd. and a member of the International Society of Ultrasound in Obstetrics and Gynecology. He also holds patents related to ultrasound processing, which are of no relevance to the Breech guidelines.
Professor DJ Murphy provides medicolegal expert opinions in Scotland and Ireland for which she is remunerated.
Dr LK Penna: None declared.
- Access the PDF version of this guideline on Wiley
- Access the web version of this guideline on Wiley
This page was last reviewed 16 March 2017.
When viewing this topic in a different language, you may notice some differences in the way the content is structured, but it still reflects the latest evidence-based guidance.

Breech presentation
- Overview
- Theory
- Diagnosis
- Management
- Follow up
- Resources
Breech presentation refers to the baby presenting for delivery with the buttocks or feet first rather than head.
Associated with increased morbidity and mortality for the mother in terms of emergency cesarean section and placenta previa; and for the baby in terms of preterm birth, small fetal size, congenital anomalies, and perinatal mortality.
Incidence decreases as pregnancy progresses and by term occurs in 3% to 4% of singleton term pregnancies.
Treatment options include external cephalic version to increase the likelihood of vaginal birth or a planned cesarean section, the optimal gestation being 37 and 39 weeks, respectively.
Planned cesarean section is considered the safest form of delivery for infants with a persisting breech presentation at term.
Breech presentation in pregnancy occurs when a baby presents with the buttocks or feet rather than the head first (cephalic presentation) and is associated with increased morbidity and mortality for both the mother and the baby. [1] Cunningham F, Gant N, Leveno K, et al. Williams obstetrics. 21st ed. New York: McGraw-Hill; 1997. [2] Kish K, Collea JV. Malpresentation and cord prolapse. In: DeCherney AH, Nathan L, eds. Current obstetric and gynecologic diagnosis and treatment. New York: McGraw-Hill Professional; 2002. There is good current evidence regarding effective management of breech presentation in late pregnancy using external cephalic version and/or planned cesarean section.
History and exam
Key diagnostic factors.
- buttocks or feet as the presenting part
- fetal head under costal margin
- fetal heartbeat above the maternal umbilicus
Other diagnostic factors
- subcostal tenderness
- pelvic or bladder pain
Risk factors
- premature fetus
- small for gestational age fetus
- nulliparity
- fetal congenital anomalies
- previous breech delivery
- uterine abnormalities
- abnormal amniotic fluid volume
- placental abnormalities
- female fetus
Diagnostic tests
1st tests to order.
- transabdominal/transvaginal ultrasound
Treatment algorithm
<37 weeks' gestation and in labor, ≥37 weeks' gestation not in labor, ≥37 weeks' gestation in labor: no imminent delivery, ≥37 weeks' gestation in labor: imminent delivery, contributors, natasha nassar, phd.
Associate Professor
Menzies Centre for Health Policy
Sydney School of Public Health
University of Sydney
Disclosures
NN has received salary support from Australian National Health and a Medical Research Council Career Development Fellowship; she is an author of a number of references cited in this topic.
Christine L. Roberts, MBBS, FAFPHM, DrPH
Research Director
Clinical and Population Health Division
Perinatal Medicine Group
Kolling Institute of Medical Research
CLR declares that she has no competing interests.
Jonathan Morris, MBChB, FRANZCOG, PhD
Professor of Obstetrics and Gynaecology and Head of Department
JM declares that he has no competing interests.
Peer reviewers
John w. bachman, md.
Consultant in Family Medicine
Department of Family Medicine
Mayo Clinic
JWB declares that he has no competing interests.
Rhona Hughes, MBChB
Lead Obstetrician
Lothian Simpson Centre for Reproductive Health
The Royal Infirmary
RH declares that she has no competing interests.
Brian Peat, MD
Director of Obstetrics
Women's and Children's Hospital
North Adelaide
South Australia
BP declares that he has no competing interests.
Lelia Duley, MBChB
Professor of Obstetric Epidemiology
University of Leeds
Bradford Institute of Health Research
Temple Bank House
Bradford Royal Infirmary
LD declares that she has no competing interests.
Justus Hofmeyr, MD
Head of the Department of Obstetrics and Gynaecology
East London Private Hospital
East London
South Africa
JH is an author of a number of references cited in this topic.
Differentials
- Transverse lie
- Caesarean birth
- Mode of term singleton breech delivery
Use of this content is subject to our disclaimer
Log in or subscribe to access all of BMJ Best Practice
Log in to access all of bmj best practice, help us improve bmj best practice.
Please complete all fields.
I have some feedback on:
We will respond to all feedback.
For any urgent enquiries please contact our customer services team who are ready to help with any problems.
Phone: +44 (0) 207 111 1105
Email: [email protected]
Your feedback has been submitted successfully.
Fetal Presentation, Position, and Lie (Including Breech Presentation)
- Key Points |
Abnormal fetal lie or presentation may occur due to fetal size, fetal anomalies, uterine structural abnormalities, multiple gestation, or other factors. Diagnosis is by examination or ultrasonography. Management is with physical maneuvers to reposition the fetus, operative vaginal delivery , or cesarean delivery .
Terms that describe the fetus in relation to the uterus, cervix, and maternal pelvis are
Fetal presentation: Fetal part that overlies the maternal pelvic inlet; vertex (cephalic), face, brow, breech, shoulder, funic (umbilical cord), or compound (more than one part, eg, shoulder and hand)
Fetal position: Relation of the presenting part to an anatomic axis; for vertex presentation, occiput anterior, occiput posterior, occiput transverse
Fetal lie: Relation of the fetus to the long axis of the uterus; longitudinal, oblique, or transverse
Normal fetal lie is longitudinal, normal presentation is vertex, and occiput anterior is the most common position.
Abnormal fetal lie, presentation, or position may occur with
Fetopelvic disproportion (fetus too large for the pelvic inlet)
Fetal congenital anomalies
Uterine structural abnormalities (eg, fibroids, synechiae)
Multiple gestation
Several common types of abnormal lie or presentation are discussed here.

Transverse lie
Fetal position is transverse, with the fetal long axis oblique or perpendicular rather than parallel to the maternal long axis. Transverse lie is often accompanied by shoulder presentation, which requires cesarean delivery.
Breech presentation
There are several types of breech presentation.
Frank breech: The fetal hips are flexed, and the knees extended (pike position).
Complete breech: The fetus seems to be sitting with hips and knees flexed.
Single or double footling presentation: One or both legs are completely extended and present before the buttocks.
Types of breech presentations
|
Breech presentation makes delivery difficult ,primarily because the presenting part is a poor dilating wedge. Having a poor dilating wedge can lead to incomplete cervical dilation, because the presenting part is narrower than the head that follows. The head, which is the part with the largest diameter, can then be trapped during delivery.
Additionally, the trapped fetal head can compress the umbilical cord if the fetal umbilicus is visible at the introitus, particularly in primiparas whose pelvic tissues have not been dilated by previous deliveries. Umbilical cord compression may cause fetal hypoxemia.

Predisposing factors for breech presentation include
Preterm labor
Uterine abnormalities
Fetal anomalies
If delivery is vaginal, breech presentation may increase risk of
Umbilical cord prolapse
Birth trauma
Perinatal death

Face or brow presentation
In face presentation, the head is hyperextended, and position is designated by the position of the chin (mentum). When the chin is posterior, the head is less likely to rotate and less likely to deliver vaginally, necessitating cesarean delivery.
Brow presentation usually converts spontaneously to vertex or face presentation.
Occiput posterior position
The most common abnormal position is occiput posterior.
The fetal neck is usually somewhat deflexed; thus, a larger diameter of the head must pass through the pelvis.
Progress may arrest in the second phase of labor. Operative vaginal delivery or cesarean delivery is often required.
Position and Presentation of the Fetus
Toward the end of pregnancy, the fetus moves into position for delivery. Normally, the presentation is vertex (head first), and the position is occiput anterior (facing toward the pregnant patient's spine) with the face and body angled to one side and the neck flexed. Abnormal presentations include face, brow, breech, and shoulder. Occiput posterior position (facing toward the pregnant patient's pubic bone) is less common than occiput anterior position. |
If a fetus is in the occiput posterior position, operative vaginal delivery or cesarean delivery is often required.
In breech presentation, the presenting part is a poor dilating wedge, which can cause the head to be trapped during delivery, often compressing the umbilical cord.
For breech presentation, usually do cesarean delivery at 39 weeks or during labor, but external cephalic version is sometimes successful before labor, usually at 37 or 38 weeks.

Copyright © 2024 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
- Cookie Preferences

Breech Presentation
- Author: Richard Fischer, MD; Chief Editor: Ronald M Ramus, MD more...
- Sections Breech Presentation
- Vaginal Breech Delivery
- Cesarean Delivery
- Comparative Studies
- External Cephalic Version
- Conclusions
- Media Gallery
Breech presentation is defined as a fetus in a longitudinal lie with the buttocks or feet closest to the cervix. This occurs in 3-4% of all deliveries. The percentage of breech deliveries decreases with advancing gestational age from 22-25% of births prior to 28 weeks' gestation to 7-15% of births at 32 weeks' gestation to 3-4% of births at term. [ 1 ]
Predisposing factors for breech presentation include prematurity , uterine malformations or fibroids, polyhydramnios , placenta previa , fetal abnormalities (eg, CNS malformations, neck masses, aneuploidy), and multiple gestations . Fetal abnormalities are observed in 17% of preterm breech deliveries and in 9% of term breech deliveries.
Perinatal mortality is increased 2- to 4-fold with breech presentation, regardless of the mode of delivery. Deaths are most often associated with malformations, prematurity, and intrauterine fetal demise .
Types of breeches
The types of breeches are as follows:
Frank breech (50-70%) - Hips flexed, knees extended (pike position)
Complete breech (5-10%) - Hips flexed, knees flexed (cannonball position)
Footling or incomplete (10-30%) - One or both hips extended, foot presenting
Historical considerations
Vaginal breech deliveries were previously the norm until 1959 when it was proposed that all breech presentations should be delivered abdominally to reduce perinatal morbidity and mortality. [ 2 ]
Vaginal breech delivery
Three types of vaginal breech deliveries are described, as follows:
Spontaneous breech delivery: No traction or manipulation of the infant is used. This occurs predominantly in very preterm, often previable, deliveries.
Assisted breech delivery: This is the most common type of vaginal breech delivery. The infant is allowed to spontaneously deliver up to the umbilicus, and then maneuvers are initiated to assist in the delivery of the remainder of the body, arms, and head.
Total breech extraction: The fetal feet are grasped, and the entire fetus is extracted. Total breech extraction should be used only for a noncephalic second twin; it should not be used for a singleton fetus because the cervix may not be adequately dilated to allow passage of the fetal head. Total breech extraction for the singleton breech is associated with a birth injury rate of 25% and a mortality rate of approximately 10%. Total breech extractions are sometimes performed by less experienced accoucheurs when a foot unexpectedly prolapses through the vagina. As long as the fetal heart rate is stable in this situation, it is permissible to manage expectantly to allow the cervix to completely dilate around the breech (see the image below).

Technique and tips for assisted vaginal breech delivery
The fetal membranes should be left intact as long as possible to act as a dilating wedge and to prevent overt cord prolapse .
Oxytocin induction and augmentation are controversial. In many previous studies, oxytocin was used for induction and augmentation, especially for hypotonic uterine dysfunction. However, others are concerned that nonphysiologic forceful contractions could result in an incompletely dilated cervix and an entrapped head.
An anesthesiologist and a pediatrician should be immediately available for all vaginal breech deliveries. A pediatrician is needed because of the higher prevalence of neonatal depression and the increased risk for unrecognized fetal anomalies. An anesthesiologist may be needed if intrapartum complications develop and the patient requires general anesthesia .
Some clinicians perform an episiotomy when the breech delivery is imminent, even in multiparas, as it may help prevent soft tissue dystocia for the aftercoming head (see the images below).

The Pinard maneuver may be needed with a frank breech to facilitate delivery of the legs but only after the fetal umbilicus has been reached. Pressure is exerted in the popliteal space of the knee. Flexion of the knee follows, and the lower leg is swept medially and out of the vagina.
No traction should be exerted on the infant until the fetal umbilicus is past the perineum, after which time maternal expulsive efforts should be used along with gentle downward and outward traction of the infant until the scapula and axilla are visible (see the image below).

Use a dry towel to wrap around the hips (not the abdomen) to help with gentle traction of the infant (see the image below).

An assistant should exert transfundal pressure from above to keep the fetal head flexed.
Once the scapula is visible, rotate the infant 90° and gently sweep the anterior arm out of the vagina by pressing on the inner aspect of the arm or elbow (see the image below).

Rotate the infant 180° in the reverse direction, and sweep the other arm out of the vagina. Once the arms are delivered, rotate the infant back 90° so that the back is anterior (see the image below).

The fetal head should be maintained in a flexed position during delivery to allow passage of the smallest diameter of the head. The flexed position can be accomplished by using the Mauriceau Smellie Veit maneuver, in which the operator's index and middle fingers lift up on the fetal maxillary prominences, while the assistant applies suprapubic pressure (see the image below).

Alternatively, Piper forceps can be used to maintain the head in a flexed position (see the image below).

In many early studies, routine use of Piper forceps was recommended to protect the head and to minimize traction on the fetal neck. Piper forceps are specialized forceps that are placed from below the infant and, unlike conventional forceps, are not tailored to the position of the fetal head (ie, it is a pelvic, not cephalic, application). The forceps are applied while the assistant supports the fetal body in a horizontal plane.
During delivery of the head, avoid extreme elevation of the body, which may result in hyperextension of the cervical spine and potential neurologic injury (see the images below).

Lower Apgar scores, especially at 1 minute, are more common with vaginal breech deliveries. Many advocate obtaining an umbilical cord artery and venous pH for all vaginal breech deliveries to document that neonatal depression is not due to perinatal acidosis.
Fetal head entrapment may result from an incompletely dilated cervix and a head that lacks time to mold to the maternal pelvis. This occurs in 0-8.5% of vaginal breech deliveries. [ 3 ] This percentage is higher with preterm fetuses (< 32 wk), when the head is larger than the body. Dührssen incisions (ie, 1-3 cervical incisions made to facilitate delivery of the head) may be necessary to relieve cervical entrapment. However, extension of the incision can occur into the lower segment of the uterus, and the operator must be equipped to deal with this complication. The Zavanelli maneuver has been described, which involves replacement of the fetus into the abdominal cavity followed by cesarean delivery. While success has been reported with this maneuver, fetal injury and even fetal death have occurred.
Nuchal arms, in which one or both arms are wrapped around the back of the neck, are present in 0-5% of vaginal breech deliveries and in 9% of breech extractions. [ 3 ] Nuchal arms may result in neonatal trauma (including brachial plexus injuries) in 25% of cases. Risks may be reduced by avoiding rapid extraction of the infant during delivery of the body. To relieve nuchal arms when it is encountered, rotate the infant so that the fetal face turns toward the maternal symphysis pubis (in the direction of the impacted arm); this reduces the tension holding the arm around the back of the fetal head, allowing for delivery of the arm.
Cervical spine injury is predominantly observed when the fetus has a hyperextended head prior to delivery. Ballas and Toaff (1976) reported 20 cases of hyperextended necks, defined as an angle of extension greater than 90° ("star-gazing"), discovered on antepartum radiographs. [ 4 ] Of the 11 fetuses delivered vaginally, 8 (73%) sustained complete cervical spinal cord lesions, defined as either transection or nonfunction.
Cord prolapse may occur in 7.4% of all breech labors. This incidence varies with the type of breech: 0-2% with frank breech, 5-10% with complete breech, and 10-25% with footling breech. [ 3 ] Cord prolapse occurs twice as often in multiparas (6%) than in primigravidas (3%). Cord prolapse may not always result in severe fetal heart rate decelerations because of the lack of presenting parts to compress the umbilical cord (ie, that which predisposes also protects).
Prior to the 2001 recommendations by the American College of Obstetricians and Gynecologists (ACOG), approximately 50% of breech presentations were considered candidates for vaginal delivery. Of these candidates, 60-82% were successfully delivered vaginally.
Candidates can be classified based on gestational age. For pregnancies prior to 26 weeks' gestation, prematurity, not mode of delivery, is the greatest risk factor. Unfortunately, no randomized clinical trials to help guide clinical management have been reported. Vaginal delivery can be considered, but a detailed discussion of the risks from prematurity and the lack of data regarding the ideal mode of delivery should take place with the parent(s). For example, intraventricular hemorrhage, which can occur in an infant of extremely low birth weight, should not be misinterpreted as proof of a traumatic vaginal breech delivery.
For pregnancies between 26 and 32 weeks, retrospective studies suggest an improved outcome with cesarean delivery, although these reports are subject to selection bias. In contrast, between 32 and 36 weeks' gestation, vaginal breech delivery may be considered after a discussion of risks and benefits with the parent(s).
After 37 weeks' gestation, parents should be informed of the results of a multicenter randomized clinical trial that demonstrated significantly increased perinatal mortality and short-term neonatal morbidity associated with vaginal breech delivery (see Comparative Studies). For those attempting vaginal delivery, if estimated fetal weight (EFW) is more than 4000 g, some recommend cesarean delivery because of concern for entrapment of the unmolded head in the maternal pelvis, although data to support this practice are limited.
A frank breech presentation is preferred when vaginal delivery is attempted. Complete breeches and footling breeches are still candidates, as long as the presenting part is well applied to the cervix and both obstetrical and anesthesia services are readily available in the event of a cord prolapse.
The fetus should show no neck hyperextension on antepartum ultrasound imaging (see the image below). Flexed or military position is acceptable.
Regarding prior cesarean delivery, a retrospective study by Ophir et al of 71 women with one prior low transverse cesarean delivery who subsequently delivered a breech fetus found that 24 women had an elective repeat cesarean and 47 women had a trial of labor. [ 5 ] In the 47 women with a trial of labor, 37 (78.7%) resulted in a vaginal delivery. Two infants in the trial of labor group had nuchal arms (1 with a transient brachial plexus injury) and 1 woman required a hysterectomy for hemorrhage due to a uterine dehiscence discovered after vaginal delivery. Vaginal breech delivery after one prior cesarean delivery is not contraindicated, though larger studies are needed.
Primigravida versus multiparous
It had been commonly believed that primigravidas with a breech presentation should have a cesarean delivery, although no data (prospective or retrospective) support this view. The only documented risk related to parity is cord prolapse, which is 2-fold higher in parous women than in primigravid women.
Radiographic and CT pelvimetry
Historically, radiograph pelvimetry was believed to be useful to quantitatively assess the inlet and mid pelvis. Recommended pelvimetry criteria included a transverse inlet diameter larger than 11.5 cm, anteroposterior inlet diameter larger than 10.5 cm, transverse midpelvic diameter (between the ischial spines) larger than 10 cm, and anteroposterior midpelvic diameter larger than 11.5 cm. However, radiographic pelvimetry is rarely, if ever, used in the United States.
CT pelvimetry , which is associated with less fetal radiation exposure than conventional radiographic pelvimetry, was more recently advocated by some investigators. It, too, is rarely used today.
Ultimately, if the obstetrical operator is not experienced or comfortable with vaginal breech deliveries, cesarean delivery may be the best choice. Unfortunately, with the dwindling number of experienced obstetricians who still perform vaginal breech deliveries and who can teach future generations of obstetricians, this technique may soon be lost due to attrition.
In 1970, approximately 14% of breeches were delivered by cesarean delivery. By 1986, that rate had increased to 86%. In 2003, based on data from the National Center for Health Statistics, the rate of cesarean delivery for all breech presentations was 87.2%. Most of the remaining breeches delivered vaginally were likely second twins, fetal demises, and precipitous deliveries. However, the rise in cesarean deliveries for breeches has not necessarily equated with an improvement in perinatal outcome. Green et al compared the outcome for term breeches prior to 1975 (595 infants, 22% cesarean delivery rate for breeches) with those from 1978-1979 (164 infants, 94% cesarean delivery rate for breeches). [ 6 ] Despite the increase in rates of cesarean delivery, the differences in rates of asphyxia, birth injury, and perinatal deaths were not significant.
Maneuvers for cesarean delivery are similar to those for vaginal breech delivery, including the Pinard maneuver, wrapping the hips with a towel for traction, head flexion during traction, rotation and sweeping out of the fetal arms, and the Mauriceau Smellie Veit maneuver.
An entrapped head can still occur during cesarean delivery as the uterus contracts after delivery of the body, even with a lower uterine segment that misleadingly appears adequate prior to uterine incision. Entrapped heads occur more commonly with preterm breeches, especially with a low transverse uterine incision. As a result, some practitioners opt to perform low vertical uterine incisions for preterm breeches prior to 32 weeks' gestation to avoid head entrapment and the kind of difficult delivery that cesarean delivery was meant to avoid. Low vertical incisions usually require extension into the corpus, resulting in cesarean delivery for all future deliveries.
If a low transverse incision is performed, the physician should move quickly once the breech is extracted in order to deliver the head before the uterus begins to contract. If any difficulty is encountered with delivery of the fetal head, the transverse incision can be extended vertically upward (T incision). Alternatively, the transverse incision can be extended laterally and upward, taking great care to avoid trauma to the uterine arteries. A third option is the use of a short-acting uterine relaxant (eg, nitroglycerin) in an attempt to facilitate delivery.
Only 3 randomized studies have evaluated the mode of delivery of the term breech. All other studies were nonrandomized or retrospective, which may be subject to selection bias.
In 1980, Collea et al randomized 208 women in labor with term frank breech presentations to either elective cesarean delivery or attempted vaginal delivery after radiographic pelvimetry. [ 7 ] Oxytocin was allowed for dysfunctional labor. Of the 60 women with adequate pelves, 49 delivered vaginally. Two neonates had transient brachial plexus injuries. Women randomized to elective cesarean delivery had higher postpartum morbidity rates (49.3% vs 6.7%).
In 1983, Gimovsky et al randomized 105 women in labor with term nonfrank breech presentations to a trial of labor versus elective cesarean delivery. [ 8 ] In this group of women, 47 had complete breech presentations, 16 had incomplete breech presentations (hips flexed, 1 knee extended/1 knee flexed), 32 had double-footling presentations, and 10 had single-footling presentations. Oxytocin was allowed for dysfunctional labor. Of the labor group, 44% had successful vaginal delivery. Most cesarean deliveries were performed for inadequate pelvic dimensions on radiographic pelvimetry. The rate of neonatal morbidity did not differ between neonates delivered vaginally and those delivered by cesarean delivery, although a higher maternal morbidity rate was noted in the cesarean delivery group.
In 2000, Hannah and colleagues completed a large, multicenter, randomized clinical trial involving 2088 term singleton fetuses in frank or complete breech presentations at 121 institutions in 26 countries. [ 9 ] In this study, popularly known as the Term Breech Trial, subjects were randomized into a planned cesarean delivery group or a planned vaginal birth group. Exclusion criteria were estimated fetal weight (EFW) more than 4000 g, hyperextension of the fetal head, lethal fetal anomaly or anomaly that might result in difficulty with delivery, or contraindication to labor or vaginal delivery (eg, placenta previa ).
Subjects randomized to cesarean delivery were scheduled to deliver after 38 weeks' gestation unless conversion to cephalic presentation had occurred. Subjects randomized to vaginal delivery were treated expectantly until labor ensued. Electronic fetal monitoring was either continuous or intermittent. Inductions were allowed for standard obstetrical indications, such as postterm gestations. Augmentation with oxytocin was allowed in the absence of apparent fetopelvic disproportion, and epidural analgesia was permitted.
Adequate labor was defined as a cervical dilation rate of 0.5 cm/h in the active phase of labor and the descent of the breech fetus to the pelvic floor within 2 hours of achieving full dilation. Vaginal delivery was spontaneous or assisted and was attended by an experienced obstetrician. Cesarean deliveries were performed for inadequate progress of labor, nonreassuring fetal heart rate, or conversion to footling breech. Results were analyzed by intent-to-treat (ie, subjects were analyzed by randomization group, not by ultimate mode of delivery).
Of 1041 subjects in the planned cesarean delivery group, 941 (90.4%) had cesarean deliveries. Of 1042 subjects in the planned vaginal delivery group, 591 (56.7%) had vaginal deliveries. Indications for cesarean delivery included: fetopelvic disproportion or failure to progress in labor (226), nonreassuring fetal heart rate tracing (129), footling breech (69), request for cesarean delivery (61), obstetrical or medical indications (45), or cord prolapse (12).
The composite measurement of either perinatal mortality or serious neonatal morbidity by 6 weeks of life was significantly lower in the planned cesarean group than in the planned vaginal group (5% vs 1.6%, P < .0001). Six of 16 neonatal deaths were associated with difficult vaginal deliveries, and 4 deaths were associated with fetal heart rate abnormalities. The reduction in risk in the cesarean group was even greater in participating countries with overall low perinatal mortality rates as reported by the World Health Organization. The difference in perinatal outcome held after controlling for the experience level of the obstetrician. No significant difference was noted in maternal mortality or serious maternal morbidity between the 2 groups within the first 6 weeks of delivery (3.9% vs 3.2%, P = .35).
A separate analysis showed no difference in breastfeeding, sexual relations, or depression at 3 months postpartum, though the reported rate of urinary incontinence was higher in the planned vaginal group (7.3% vs 4.5%).
Based on the multicenter trial, the ACOG published a Committee Opinion in 2001 that stated "planned vaginal delivery of a singleton term breech may no longer be appropriate." This did not apply to those gravidas presenting in advanced labor with a term breech and imminent delivery or to a nonvertex second twin.
A follow-up study by Whyte et al was conducted in 2004 on 923 children who were part of the initial multicenter study. [ 10 ] The authors found no differences between the planned cesarean delivery and planned vaginal breech delivery groups with regards to infant death rates or neurodevelopmental delay by age 2 years. Similarly, among 917 participating mothers from the original trial, no substantive differences were apparent in maternal outcome between the 2 groups. [ 11 ] No longer-term maternal effects, such as the impact of a uterine scar on future pregnancies, have yet been reported.
A meta-analysis of the 3 above mentioned randomized trials was published in 2015. The findings included a reduction in perinatal/neonatal death, reduced composite short-term outcome of perinatal/neonatal death or serious neonatal morbidity with planned cesarean delivery versus planned vaginal delivery. [ 12 ] However, at 2 years of age, there was no significant difference in death or neurodevelopmental delay between the two groups. Maternal outcomes assessed at 2 years after delivery were not significantly different.
With regard to preterm breech deliveries, only one prospective randomized study has been performed, which included only 38 subjects (28-36 wk) with preterm labor and breech presentation. [ 13 ] Of these subjects, 20 were randomized to attempted vaginal delivery and 18 were randomized to immediate cesarean delivery. Of the attempted vaginal delivery group, 25% underwent cesarean delivery for nonreassuring fetal heart rate tracings. Five neonatal deaths occurred in the vaginal delivery group, and 1 neonatal death occurred in the cesarean delivery group. Two neonates died from fetal anomalies, 3 from respiratory distress, and 1 from sepsis.
Nonanomalous infants who died were not acidotic at delivery and did not have birth trauma. Differences in Apgar scores were not significant, although the vaginal delivery group had lower scores. The small number of enrolled subjects precluded any definitive conclusions regarding the safety of vaginal breech delivery for a preterm breech.
Retrospective analyses showed a higher mortality rate in vaginal breech neonates weighing 750-1500 g (26-32 wk), but less certain benefit was shown with cesarean delivery if the fetal weight was more than 1500 g (approximately 32 wk). Therefore, this subgroup of very preterm infants (26-32 wk) may benefit from cesarean delivery, although this recommendation is based on potentially biased retrospective data.
A large cohort study was published in 2015 from the Netherlands Perinatal Registry, which included 8356 women with a preterm (26-36 6/7 weeks) breech from 2000 to 2011, over three quarters of whom intended to deliver vaginally. In this overall cohort, there was no significant difference in perinatal mortality between the planned vaginal delivery and planned cesarean delivery groups (adjusted odds ratio 0.97, 95% confidence interval 0.60 – 1.57). However, the subgroup delivering at 28 to 32 weeks had a lower perinatal mortality with planned cesarean section (aOR 0.27, 95% CI 0.10 – 0.77). After adding a composite of perinatal morbidity, planned cesarean delivery was associated with a better outcome than a planned vaginal delivery (aOR 0.77, 95% CI 0.63 – 0.93. [ 14 ]
A Danish study found that nulliparous women with a singleton breech presentation who had a planned vaginal delivery were at significantly higher risk for postoperative complications, such as infection, compared with women who had a planned cesarean delivery. This increased risk was due to the likelihood of conversion to an emergency cesarean section, which occurred in over 69% of the planned vaginal deliveries in the study. [ 15 ]
The Maternal-Fetal Medicine Units Network of the US National Institute of Child Health and Human Development considered a multicenter randomized clinical trial of attempted vaginal delivery versus elective cesarean delivery for 24- to 28-week breech fetuses. [ 16 ] However, it was not initiated because of anticipated difficulty with recruitment, inadequate numbers to show statistically significant differences, and medicolegal concerns. Therefore, this study is not likely to be performed.
External cephalic version (ECV) is the transabdominal manual rotation of the fetus into a cephalic presentation.
Initially popular in the 1960s and 1970s, ECV virtually disappeared after reports of fetal deaths following the procedure. Reintroduced to the United States in the 1980s, it became increasingly popular in the 1990s.
Improved outcome may be related to the use of nonstress tests both before and after ECV, improved selection of low-risk fetuses, and Rh immune globulin to prevent isoimmunization.
Prepare for the possibility of cesarean delivery. Obtain a type and screen as well as an anesthesia consult. The patient should have nothing by mouth for at least 8 hours prior to the procedure. Recent ultrasonography should have been performed for fetal position, to check growth and amniotic fluid volume, to rule out a placenta previa, and to rule out anomalies associated with breech. Another sonogram should be performed on the day of the procedure to confirm that the fetus is still breech.
A nonstress test (biophysical profile as backup) should be performed prior to ECV to confirm fetal well-being.
Perform ECV in or near a delivery suite in the unlikely event of fetal compromise during or following the procedure, which may require emergent delivery.
ECV can be performed with 1 or 2 operators. Some prefer to have an assistant to help turn the fetus, elevate the breech out of the pelvis, or to monitor the position of the baby with ultrasonography. Others prefer a single operator approach, as there may be better coordination between the forces that are raising the breech and moving the head.
ECV is accomplished by judicious manipulation of the fetal head toward the pelvis while the breech is brought up toward the fundus. Attempt a forward roll first and then a backward roll if the initial attempts are unsuccessful. No consensus has been reached regarding how many ECV attempts are appropriate at one time. Excessive force should not be used at any time, as this may increase the risk of fetal trauma.
Following an ECV attempt, whether successful or not, repeat the nonstress test (biophysical profile if needed) prior to discharge. Also, administer Rh immune globulin to women who are Rh negative. Some physicians traditionally induce labor following successful ECV. However, as virtually all of these recently converted fetuses are unengaged, many practitioners will discharge the patient and wait for spontaneous labor to ensue, thereby avoiding the risk of a failed induction of labor. Additionally, as most ECV’s are attempted prior to 39 weeks, as long as there are no obstetrical or medical indications for induction, discharging the patient to await spontaneous labor would seem most prudent.
In those with an unsuccessful ECV, the practitioner has the option of sending the patient home or proceeding with a cesarean delivery. Expectant management allows for the possibility of spontaneous version. Alternatively, cesarean delivery may be performed at the time of the failed ECV, especially if regional anesthesia is used and the patient is already in the delivery room (see Regional anesthesia). This would minimize the risk of a second regional analgesia.
In those with an unsuccessful ECV, the practitioner may send the patient home, if less than 39 weeks, with plans for either a vaginal breech delivery or scheduled cesarean after 39 weeks. Expectant management allows for the possibility of a spontaneous version. Alternatively, if ECV is attempted after 39 weeks, cesarean delivery may be performed at the time of the failed ECV, especially if regional anesthesia is used and the patient is already in the delivery room (see Regional anesthesia). This would minimize the risk of a second regional analgesia.
Success rate
Success rates vary widely but range from 35% to 86% (average success rate in the 2004 National Vital Statistics was 58%). Improved success rates occur with multiparity, earlier gestational age, frank (versus complete or footling) breech presentation, transverse lie, and in African American patients.
Opinions differ regarding the influence of maternal weight, placental position, and amniotic fluid volume. Some practitioners find that thinner patients, posterior placentas, and adequate fluid volumes facilitate successful ECV. However, both patients and physicians need to be prepared for an unsuccessful ECV; version failure is not necessarily a reflection of the skill of the practitioner.
Zhang et al reviewed 25 studies of ECV in the United States, Europe, Africa, and Israel. [ 17 ] The average success rate in the United States was 65%. Of successful ECVs, 2.5% reverted back to breech presentation (other estimates range from 3% to 5%), while 2% of unsuccessful ECVs had spontaneous version to cephalic presentation prior to labor (other estimates range from 12% to 26%). Spontaneous version rates depend on the gestational age when the breech is discovered, with earlier breeches more likely to undergo spontaneous version.
A prospective study conducted in Germany by Zielbauer et al demonstrated an overall success rate of 22.4% for ECV among 353 patients with a singleton fetus in breech presentation. ECV was performed at 38 weeks of gestation. Factors found to increase the likelihood of success were a later week of gestation, abundant amniotic fluid, fundal and anterior placental location, and an oblique lie. [ 18 ]
A systematic review in 2015 looked at the effectiveness of ECV with eight randomized trials of ECV at term. Compared to women with no attempt at ECV, ECV reduced non-cephalic presentation at birth by 60% and reduced cesarean sections by 40% in the same group. [ 19 ] Although the rate of cesarean section is lower when ECV is performed than if not, the overall rate of cesarean section remains nearly twice as high after successful ECV due to both dystocia and non-reassuring fetal heart rate patterns. [ 20 ] Nulliparity was the only factor shown in follow-up to increase the risk of instrumental delivery following successful ECV. [ 21 ]
While most studies of ECV have been performed in university hospitals, Cook showed that ECV has also been effective in the private practice setting. [ 22 ] Of 65 patients with term breeches, 60 were offered ECV. ECV was successful in 32 (53%) of the 60 patients, with vaginal delivery in 23 (72%) of the 32 patients. Of the remaining breech fetuses believed to be candidates for vaginal delivery, 8 (80%) had successful vaginal delivery. The overall vaginal delivery rate was 48% (31 of 65 patients), with no significant morbidity.
Cost analysis
In 1995, Gifford et al performed a cost analysis of 4 options for breech presentations at term: (1) ECV attempt on all breeches, with attempted vaginal breech delivery for selected persistent breeches; (2) ECV on all breeches, with cesarean delivery for persistent breeches; (3) trial of labor for selected breeches, with scheduled cesarean delivery for all others; and (4) scheduled cesarean delivery for all breeches prior to labor. [ 23 ]
ECV attempt on all breeches with attempted vaginal breech delivery on selected persistent breeches was associated with the lowest cesarean delivery rate and was the most cost-effective approach. The second most cost-effective approach was ECV attempt on all breeches, with cesarean delivery for persistent breeches.
Uncommon risks of ECV include fractured fetal bones, precipitation of labor or premature rupture of membranes , abruptio placentae , fetomaternal hemorrhage (0-5%), and cord entanglement (< 1.5%). A more common risk of ECV is transient slowing of the fetal heart rate (in as many as 40% of cases). This risk is believed to be a vagal response to head compression with ECV. It usually resolves within a few minutes after cessation of the ECV attempt and is not usually associated with adverse sequelae for the fetus.
Trials have not been large enough to determine whether the overall risk of perinatal mortality is increased with ECV. The Cochrane review from 2015 reported perinatal death in 2 of 644 in ECV and 6 of 661 in the group that did not attempt ECV. [ 19 ]
A 2016 Practice Bulletin by ACOG recommended that all women who are near term with breech presentations should be offered an ECV attempt if there are no contraindications (see Contraindications below). [ 24 ] ACOG guidelines issued in 2020 recommend that ECV should be performed starting at 37+0 weeks, in order to reduce the likelihood of reversion and to increase the rate of spontaneous version. [ 25 ]
ACOG recommends that ECV be offered as an alternative to a planned cesarean section for a patient who has a term singleton breech fetus, wishes to have a planned vaginal delivery of a vertex-presenting fetus, and has no contraindications. ACOG also advises that ECV be attempted only in settings where cesarean delivery services are available. [ 26 ]
ECV is usually not performed on preterm breeches because they are more likely to undergo spontaneous version to cephalic presentation and are more likely to revert to breech after successful ECV (approximately 50%). Earlier studies of preterm ECV did not show a difference in the rates of breech presentations at term or overall rates of cesarean delivery. Additionally, if complications of ECV were to arise that warranted emergent delivery, it would result in a preterm neonate with its inherent risks. The Early External Cephalic Version (ECV) 2 trial was an international, multicentered, randomized clinical trial that compared ECV performed at 34-35 weeks’ gestation compared with 37 weeks’ gestation or more. [ 27 ] Early ECV increased the chance of cephalic presentation at birth; however, no difference in cesarean delivery rates was noted, along with a nonstatistical increase in preterm births.
A systematic review looked at 5 studies of ECV completed prior to 37 weeks and concluded that compared with no ECV attempt, ECV commenced before term reduces the non-cephalic presentation at birth, however early ECV may increase the risk of late preterm birth. [ 28 ]
Given the increasing awareness of the risks of late preterm birth and early term deliveries, the higher success of earlier ECV should be weighed against the risks of iatrogenic prematurity should a complication arise necessitating delivery.
Contraindications
Absolute contraindications for ECV include multiple gestations with a breech presenting fetus, contraindications to vaginal delivery (eg, herpes simplex virus infection, placenta previa), and nonreassuring fetal heart rate tracing.
Relative contraindications include polyhydramnios or oligohydramnios , fetal growth restriction , uterine malformation , and major fetal anomaly.
Controversial candidates
Women with prior uterine incisions may be candidates for ECV, but data are scant. In 1991, Flamm et al attempted ECV on 56 women with one or more prior low transverse cesarean deliveries. [ 29 ] The success rate of ECV was 82%, with successful vaginal births in 65% of patients with successful ECVs. No uterine ruptures occurred during attempted ECV or subsequent labor, and no significant fetal complications occurred.
In 2010 ACOG acknowledged that although there is limited data in both the above study and one more recently, [ 30 ] no serious adverse events occurred in these series. A larger prospective cohort study that was published in 2014 reported similar success rates of ECV among women with and without prior cesarean section, although lower vaginal birth rates. There were, however, no cases of uterine rupture or other adverse outcomes. [ 31 ]
Another controversial area is performing ECV on a woman in active labor. In 1985, Ferguson and Dyson reported on 15 women in labor with term breeches and intact membranes. [ 32 ] Four patients were dilated greater than 5 cm (2 women were dilated 8 cm). Tocolysis was administered, and intrapartum ECV was attempted. ECV was successful in 11 of 15 patients, with successful vaginal births in 10 patients. No adverse effects were noted. Further studies are needed to evaluate the safety and efficacy of intrapartum ECV.
Data regarding the benefit of intravenous or subcutaneous beta-mimetics in improving ECV rates are conflicting.
In 1996, Marquette et al performed a prospective, randomized, double-blinded study on 283 subjects with breech presentations between 36 and 41 weeks' gestation. [ 33 ] Subjects received either intravenous ritodrine or placebo. The success rate of ECV was 52% in the ritodrine group versus 42% in the placebo group ( P = .35). When only nulliparous subjects were analyzed, significant differences were observed in the success of ECV (43% vs 25%, P < .03). ECV success rates were significantly higher in parous versus nulliparous subjects (61% vs 34%, P < .0001), with no additional improvement with ritodrine.
A systematic review published in 2015 of six randomized controlled trials of ECV that compared the use of parenteral beta-mimetic tocolysis during ECV concluded that tocolysis was effective in increasing the rate of cephalic presentation in labor and reducing the cesarean delivery rate by almost 25% in both nulliparous and multiparous women. [ 34 ] Data on adverse effects and other tocolytics was insufficient. A review published in 2011 on Nifedipine did not show an improvement in ECV success. [ 35 ]
Regional anesthesia
Regional analgesia, either epidural or spinal, may be used to facilitate external cephalic version (ECV) success. When analgesia levels similar to that for cesarean delivery are given, it allows relaxation of the anterior abdominal wall, making palpation and manipulation of the fetal head easier. Epidural or spinal analgesia also eliminates maternal pain that may cause bearing down and tensing of the abdominal muscles. If ECV is successful, the epidural can be removed and the patient sent home to await spontaneous labor. If ECV is unsuccessful, a patient can proceed to cesarean delivery under her current anesthesia, if the gestational age is more than 39 weeks.
The main disadvantage is the inherent risk of regional analgesia, which is considered small. Additionally, lack of maternal pain could potentially result in excessive force being applied to the fetus without the knowledge of the operator.
In 1994, Carlan et al retrospectively analyzed 61 women who were at more than 36 weeks' gestation and had ECV with or without epidural. [ 36 ] The success rate of ECV was 59% in the epidural group and 24% in the nonepidural group ( P < .05). In 7 of 8 women with unsuccessful ECV without epidural, a repeat ECV attempt after epidural was successful. No adverse effects on maternal or perinatal morbidity or mortality occurred.
In 1997, Schorr et al randomized 69 subjects who were at least 37 weeks' gestation to either epidural or control groups prior to attempted ECV. [ 37 ] Those in whom ECV failed underwent cesarean delivery. The success rate of ECV was 69% in the epidural group and 32% in the control group (RR, 2.12; 95% CI, 1.24-3.62). The cesarean delivery rate was 79% in the control group and 34% in the epidural group ( P = .001). No complications of epidural anesthesia and no adverse fetal effects occurred.
In 1999, Dugoff et al randomized 102 subjects who were at more than 36 weeks' gestation with breech presentations to either spinal anesthesia or a control group. [ 38 ] All subjects received 0.25 mg terbutaline subcutaneously. The success rate of ECV was 44% in the spinal group and 42% in the nonspinal group, which was not statistically significant.
In contrast, a 2007 randomized clinical trial of spinal analgesia versus no analgesia in 74 women showed a significant improvement in ECV success (66.7% vs 32.4%, p = .004), with a significantly lower pain score by the patient. [ 39 ]
The 2015 systematic review asserted that regional analgesia in combination with a tocolytic was more effective than the tocolytic alone for increasing ECV success; however there was no difference in cephalic presentation in labor. Data from the same review was insufficient to assess regional analgesia without tocolysis [ 34 ]
Acoustic stimulation
Johnson and Elliott performed a randomized, blinded trial on 23 subjects to compare acoustic stimulation prior to ECV with a control group when the fetal spine was in the midline (directly back up or back down). [ 40 ] Of those who received acoustic stimulation, 12 of 12 fetuses shifted to a spine-lateral position after acoustic stimulation, and 11 (91%) underwent successful ECV. In the control group, 0 of 11 shifts and 1 (9%) successful ECV ( P < .0001) occurred. Additional studies are needed.
Amnioinfusion
Although an earlier study reported on the utility of amnioinfusion to successfully turn 6 fetuses who initially failed ECV, [ 41 ] a subsequent study was published of 7 women with failed ECV who underwent amniocentesis and amnioinfusion of up to 1 liter of crystalloid. [ 42 ] Repeat attempts of ECV were unsuccessful in all 7 cases. Amnioinfusion to facilitate ECV cannot be recommended at this time.
Vaginal delivery rates after successful version
The rate of cesarean delivery ranges from 0-31% after successful external cephalic version (ECV). Controversy has existed on whether there is a higher rate of cesarean delivery for labor dystocia following ECV. In 1994, a retrospective study by Egge et al of 76 successful ECVs matched with cephalic controls by delivery date, parity, and gestational age failed to note any significant difference in the cesarean delivery rate (8% in ECV group, 6% in control group). [ 43 ]
However, in 1997, Lau et al compared 154 successful ECVs to 308 spontaneously occurring cephalic controls (matched for age, parity, and type of labor onset) with regard to the cesarean delivery rate. [ 44 ] Cesarean delivery rates were higher after ECV (16.9% vs 7.5%, P < .005) because of higher rates of cephalopelvic disproportion and nonreassuring fetal heart rate tracings. This may be related to an increased frequency of compound presentations after ECV. Immediate induction of labor after successful ECV may also contribute to an increase in the cesarean delivery rate due to failed induction in women with unripe cervices and unengaged fetal heads.
Further, in another cohort study from 2015, factors were described which decreased the vaginal delivery rate after successful ECV including labor induction, less than 2 weeks between ECV and delivery, high body mass index, and previous cesarean. [ 45 ] The overall caesarean delivery rate in this cohort was 15%.
Vaginal breech delivery requires an experienced obstetrician and careful counseling of the parents. Although studies on the delivery of the preterm breech are limited, the multicenter Term Breech Trial found an increased rate of perinatal mortality and serious immediate perinatal morbidity, though no differences were seen in infant outcome at 2 years of age.
Parents must be informed about potential risks and benefits to the mother and neonate for both vaginal breech delivery and cesarean delivery. Discussion of risks should not be limited only to the current pregnancy. The risks of a cesarean on subsequent pregnancies, including uterine rupture and placental attachment abnormalities ( placenta previa , abruption , accreta), as well as maternal and perinatal sequelae from these complications, should be reviewed as well.
It remains concerning that the dearth of experienced physicians to teach younger practitioners will lead to the abandonment of vaginal breeches altogether. For those wishing to learn the art of vaginal breech deliveries, simulation training with pelvic models has been advocated to familiarize trainees with the procedure in a nonthreatening environment. [ 46 ] Once comfortable with the appropriate maneuvers, vaginal delivery of the second, noncephalic twin, may be attempted under close supervision by an experienced physician. The cervix will already be fully dilated, and, assuming the second twin is not significantly larger, the successful vaginal delivery rate has been quoted to be as high as 96%.
External cephalic version (ECV) is a safe alternative to vaginal breech delivery or cesarean delivery, reducing the cesarean delivery rate for breech by 50%. ACOG recommends offering ECV to all women with a breech fetus near term. [ 24 ] Adjuncts such as tocolysis, regional anesthesia, and acoustic stimulation when appropriate may improve ECV success rates.
Hickok DE, Gordon DC, Milberg JA, Williams MA, Daling JR. The frequency of breech presentation by gestational age at birth: a large population-based study. Am J Obstet Gynecol . 1992 Mar. 166(3):851-2. [QxMD MEDLINE Link] .
Wright RC. Reduction of perinatal mortality and morbidity in breech delivery through routine use of cesarean section. Obstet Gynecol . 1959. 14:758-63.
Cheng M, Hannah M. Breech delivery at term: a critical review of the literature. Obstet Gynecol . 1993 Oct. 82(4 Pt 1):605-18. [QxMD MEDLINE Link] .
Ballas S, Toaff R. Hyperextension of the fetal head in breech presentation: radiological evaluation and significance. Br J Obstet Gynaecol . 1976 Mar. 83(3):201-4. [QxMD MEDLINE Link] .
Ophir E, Oettinger M, Yagoda A, Markovits Y, Rojansky N, Shapiro H. Breech presentation after cesarean section: always a section?. Am J Obstet Gynecol . 1989 Jul. 161(1):25-8. [QxMD MEDLINE Link] .
Green JE, McLean F, Smith LP, Usher R. Has an increased cesarean section rate for term breech delivery reduced in incidence of birth asphyxia, trauma, and death?. Am J Obstet Gynecol . 1982 Mar 15. 142(6 Pt 1):643-8. [QxMD MEDLINE Link] .
Collea JV, Chein C, Quilligan EJ. The randomized management of term frank breech presentation: a study of 208 cases. Am J Obstet Gynecol . 1980 May 15. 137(2):235-44. [QxMD MEDLINE Link] .
Gimovsky ML, Wallace RL, Schifrin BS, Paul RH. Randomized management of the nonfrank breech presentation at term: a preliminary report. Am J Obstet Gynecol . 1983 May 1. 146(1):34-40. [QxMD MEDLINE Link] .
Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Term Breech Trial Collaborative Group. Lancet . 2000 Oct 21. 356(9239):1375-83. [QxMD MEDLINE Link] .
Whyte H, Hannah ME, Saigal S, et al. Outcomes of children at 2 years after planned cesarean birth versus planned vaginal birth for breech presentation at term: the International Randomized Term Breech Trial. Am J Obstet Gynecol . 2004 Sep. 191(3):864-71. [QxMD MEDLINE Link] .
Hannah ME, Whyte H, Hannah WJ, Hewson S, Amankwah K, Cheng M. Maternal outcomes at 2 years after planned cesarean section versus planned vaginal birth for breech presentation at term: the international randomized Term Breech Trial. Am J Obstet Gynecol . 2004 Sep. 191(3):917-27. [QxMD MEDLINE Link] .
Hofmeyr GJ, Hannah M, Lawrie TA. Planned caesarean section for term breech delivery. Cochrane Database Syst Rev . 2015 Jul 21. 7:CD000166. [QxMD MEDLINE Link] .
Zlatnik FJ. The Iowa premature breech trial. Am J Perinatol . 1993 Jan. 10(1):60-3. [QxMD MEDLINE Link] .
Bergenhenegouwen L, Vlemmix F, Ensing S, Schaaf J, van der Post J, Abu-Hanna A, et al. Preterm Breech Presentation: A Comparison of Intended Vaginal and Intended Cesarean Delivery. Obstet Gynecol . 2015 Dec. 126 (6):1223-30. [QxMD MEDLINE Link] .
Caning MM, Rasmussen SC, Krebs L. Maternal outcomes of planned mode of delivery for term breech in nulliparous women. PLoS One . 2024. 19 (4):e0297971. [QxMD MEDLINE Link] . [Full Text] .
Eller DP, VanDorsten JP. Route of delivery for the breech presentation: a conundrum. Am J Obstet Gynecol . 1995 Aug. 173(2):393-6; discussion 396-8. [QxMD MEDLINE Link] .
Zhang J, Bowes WA Jr, Fortney JA. Efficacy of external cephalic version: a review. Obstet Gynecol . 1993 Aug. 82(2):306-12. [QxMD MEDLINE Link] .
Zielbauer AS, Louwen F, Jennewein L. External cephalic version at 38 weeks' gestation at a specialized German single center. PLoS One . 2021. 16 (8):e0252702. [QxMD MEDLINE Link] . [Full Text] .
Hofmeyr GJ, Kulier R, West HM. External cephalic version for breech presentation at term. Cochrane Database Syst Rev . 2015 Apr 1. 4:CD000083. [QxMD MEDLINE Link] .
de Hundt M, Velzel J, de Groot CJ, Mol BW, Kok M. Mode of delivery after successful external cephalic version: a systematic review and meta-analysis. Obstet Gynecol . 2014 Jun. 123 (6):1327-34. [QxMD MEDLINE Link] .
de Hundt M, Vlemmix F, Bais JM, de Groot CJ, Mol BW, Kok M. Risk factors for cesarean section and instrumental vaginal delivery after successful external cephalic version. J Matern Fetal Neonatal Med . 2016 Jun. 29 (12):2005-7. [QxMD MEDLINE Link] .
Cook HA. Experience with external cephalic version and selective vaginal breech delivery in private practice. Am J Obstet Gynecol . 1993 Jun. 168(6 Pt 1):1886-9; discussion 1889-90. [QxMD MEDLINE Link] .
Gifford DS, Keeler E, Kahn KL. Reductions in cost and cesarean rate by routine use of external cephalic version: a decision analysis. Obstet Gynecol . 1995 Jun. 85(6):930-6. [QxMD MEDLINE Link] .
Practice Bulletin No. 161 Summary: External Cephalic Version. Obstet Gynecol . 2016 Feb. 127 (2):412-3. [QxMD MEDLINE Link] .
[Guideline] External Cephalic Version: ACOG Practice Bulletin, Number 221. Obstet Gynecol . 2020 May. 135 (5):e203-e212. [QxMD MEDLINE Link] .
[Guideline] ACOG Committee Opinion No. 745: Mode of Term Singleton Breech Delivery. Obstet Gynecol . 2018 Aug; reaffirmed 2023. 132 (2):e60-e63. [QxMD MEDLINE Link] . [Full Text] .
Hutton E, Hannah M, Ross S, Delisle MF, Carson G, Windrim R, et al. The Early External Cephalic Version (ECV) 2 Trial: an international multicentre randomised controlled trial of timing of ECV for breech pregnancies. BJOG . 2011 Apr. 118(5):564-577. [QxMD MEDLINE Link] .
Hutton EK, Hofmeyr GJ, Dowswell T. External cephalic version for breech presentation before term. Cochrane Database Syst Rev . 2015 Jul 29. 7:CD000084. [QxMD MEDLINE Link] .
Flamm BL, Fried MW, Lonky NM, Giles WS. External cephalic version after previous cesarean section. Am J Obstet Gynecol . 1991 Aug. 165(2):370-2. [QxMD MEDLINE Link] .
de Meeus JB, Ellia F, Magnin G. External cephalic version after previous cesarean section: a series of 38 cases. Eur J Obstet Gynecol Reprod Biol . 1998 Oct. 81 (1):65-8. [QxMD MEDLINE Link] .
Burgos J, Cobos P, Rodríguez L, Osuna C, Centeno MM, Martínez-Astorquiza T, et al. Is external cephalic version at term contraindicated in previous caesarean section? A prospective comparative cohort study. BJOG . 2014 Jan. 121 (2):230-5; discussion 235. [QxMD MEDLINE Link] .
Ferguson JE 2nd, Dyson DC. Intrapartum external cephalic version. Am J Obstet Gynecol . 1985 Jun 1. 152(3):297-8. [QxMD MEDLINE Link] .
Marquette GP, Boucher M, Theriault D, Rinfret D. Does the use of a tocolytic agent affect the success rate of external cephalic version?. Am J Obstet Gynecol . 1996 Oct. 175(4 Pt 1):859-61. [QxMD MEDLINE Link] .
Cluver C, Gyte GM, Sinclair M, Dowswell T, Hofmeyr GJ. Interventions for helping to turn term breech babies to head first presentation when using external cephalic version. Cochrane Database Syst Rev . 2015 Feb 9. 2:CD000184. [QxMD MEDLINE Link] .
Wilcox CB, Nassar N, Roberts CL. Effectiveness of nifedipine tocolysis to facilitate external cephalic version: a systematic review. BJOG . 2011 Mar. 118 (4):423-8. [QxMD MEDLINE Link] .
Carlan SJ, Dent JM, Huckaby T, Whittington EC, Shaefer D. The effect of epidural anesthesia on safety and success of external cephalic version at term. Anesth Analg . 1994 Sep. 79(3):525-8. [QxMD MEDLINE Link] .
Schorr SJ, Speights SE, Ross EL, et al. A randomized trial of epidural anesthesia to improve external cephalic version success. Am J Obstet Gynecol . 1997 Nov. 177(5):1133-7. [QxMD MEDLINE Link] .
Dugoff L, Stamm CA, Jones OW 3rd, Mohling SI, Hawkins JL. The effect of spinal anesthesia on the success rate of external cephalic version: a randomized trial. Obstet Gynecol . 1999 Mar. 93(3):345-9. [QxMD MEDLINE Link] .
Weiniger CF, Ginosar Y, Elchalal U, Sharon E, Nokrian M, Ezra Y. External cephalic version for breech presentation with or without spinal analgesia in nulliparous women at term: a randomized controlled trial. Obstet Gynecol . 2007 Dec. 110(6):1343-50. [QxMD MEDLINE Link] .
Johnson RL, Elliott JP. Fetal acoustic stimulation, an adjunct to external cephalic version: a blinded, randomized crossover study. Am J Obstet Gynecol . 1995 Nov. 173(5):1369-72. [QxMD MEDLINE Link] .
Benifla JL, Goffinet F, Darai E, Madelenat P. Antepartum transabdominal amnioinfusion to facilitate external cephalic version after initial failure. Obstet Gynecol . 1994 Dec. 84(6):1041-2. [QxMD MEDLINE Link] .
Adama van Scheltema PN, Feitsma AH, Middeldorp JM, Vandenbussche FP, Oepkes D. Amnioinfusion to facilitate external cephalic version after initial failure. Obstet Gynecol . 2006 Sep. 108(3 Pt 1):591-2. [QxMD MEDLINE Link] .
Egge T, Schauberger C, Schaper A. Dysfunctional labor after external cephalic version. Obstet Gynecol . 1994 May. 83(5 Pt 1):771-3. [QxMD MEDLINE Link] .
Lau TK, Lo KW, Rogers M. Pregnancy outcome after successful external cephalic version for breech presentation at term. Am J Obstet Gynecol . 1997 Jan. 176(1 Pt 1):218-23. [QxMD MEDLINE Link] .
Burgos J, Iglesias M, Pijoan JI, Rodriguez L, Fernández-Llebrez L, Martínez-Astorquiza T. Probability of cesarean delivery after successful external cephalic version. Int J Gynaecol Obstet . 2015 Nov. 131 (2):192-5. [QxMD MEDLINE Link] .
Deering S, Brown J, Hodor J, Satin AJ. Simulation training and resident performance of singleton vaginal breech delivery. Obstet Gynecol . 2006 Jan. 107(1):86-9. [QxMD MEDLINE Link] .
- Footling breech presentation. Once the feet have delivered, one may be tempted to pull on the feet. However, a singleton gestation should not be pulled by the feet because this action may precipitate head entrapment in an incompletely dilated cervix or may precipitate nuchal arms. As long as the fetal heart rate is stable and no physical evidence of a prolapsed cord is evident, management may be expectant while awaiting full cervical dilation.
- Assisted vaginal breech delivery. Thick meconium passage is common as the breech is squeezed through the birth canal. This is usually not associated with meconium aspiration because the meconium passes out of the vagina and does not mix with the amniotic fluid.
- Assisted vaginal breech delivery. The Ritgen maneuver is applied to take pressure off the perineum during vaginal delivery. Episiotomies are often performed for assisted vaginal breech deliveries, even in multiparous women, to prevent soft tissue dystocia.
- Assisted vaginal breech delivery. No downward or outward traction is applied to the fetus until the umbilicus has been reached.
- Assisted vaginal breech delivery. With a towel wrapped around the fetal hips, gentle downward and outward traction is applied in conjunction with maternal expulsive efforts until the scapula is reached. An assistant should be applying gentle fundal pressure to keep the fetal head flexed.
- Assisted vaginal breech delivery. After the scapula is reached, the fetus should be rotated 90° in order to deliver the anterior arm.
- Assisted vaginal breech delivery. The anterior arm is followed to the elbow, and the arm is swept out of the vagina.
- Assisted vaginal breech delivery. The fetus is rotated 180°, and the contralateral arm is delivered in a similar manner as the first. The infant is then rotated 90° to the backup position in preparation for delivery of the head.
- Assisted vaginal breech delivery. The fetal head is maintained in a flexed position by using the Mauriceau maneuver, which is performed by placing the index and middle fingers over the maxillary prominence on either side of the nose. The fetal body is supported in a neutral position, with care to not overextend the neck.
- Piper forceps application. Piper forceps are specialized forceps used only for the after-coming head of a breech presentation. They are used to keep the fetal head flexed during extraction of the head. An assistant is needed to hold the infant while the operator gets on one knee to apply the forceps from below.
- Assisted vaginal breech delivery. Low 1-minute Apgar scores are not uncommon after a vaginal breech delivery. A pediatrician should be present for the delivery in the event that neonatal resuscitation is needed.
- Assisted vaginal breech delivery. The neonate after birth.
- Ultrasound demonstrating a fetus in breech presentation with a hyperextended head (ie, "star gazing").

Contributor Information and Disclosures
Richard Fischer, MD Professor, Division Head, Department of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, Cooper University Hospital Richard Fischer, MD is a member of the following medical societies: American College of Obstetricians and Gynecologists , American Institute of Ultrasound in Medicine , Association of Professors of Gynecology and Obstetrics , Society for Maternal-Fetal Medicine Disclosure: Stock ownership for: Pfizer Pharmaceuticals (< 5% of portfolio); Johnson & Johnson (< 5% of portfolio).
Alisa B Modena, MD, FACOG Assistant Professor, Cooper Medical School of Rowan University; Attending Physician, Division of Maternal-Fetal Medicine, Cooper University Hospital Alisa B Modena, MD, FACOG is a member of the following medical societies: American College of Obstetricians and Gynecologists , American Institute of Ultrasound in Medicine , Philadelphia Perinatal Society, Society for Maternal-Fetal Medicine Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference Disclosure: Received salary from Medscape for employment. for: Medscape.
Richard S Legro, MD Professor, Department of Obstetrics and Gynecology, Division of Reproductive Endocrinology, Pennsylvania State University College of Medicine; Consulting Staff, Milton S Hershey Medical Center Richard S Legro, MD is a member of the following medical societies: American College of Obstetricians and Gynecologists , Society of Reproductive Surgeons , American Society for Reproductive Medicine , Endocrine Society , Phi Beta Kappa Disclosure: Received honoraria from Korea National Institute of Health and National Institute of Health (Bethesda, MD) for speaking and teaching; Received honoraria from Greater Toronto Area Reproductive Medicine Society (Toronto, ON, CA) for speaking and teaching; Received honoraria from American College of Obstetrics and Gynecologists (Washington, DC) for speaking and teaching; Received honoraria from National Institute of Child Health and Human Development Pediatric and Adolescent Gynecology Research Thi.
Ronald M Ramus, MD Professor of Obstetrics and Gynecology, Director, Division of Maternal-Fetal Medicine, Virginia Commonwealth University School of Medicine Ronald M Ramus, MD is a member of the following medical societies: American College of Obstetricians and Gynecologists , American Institute of Ultrasound in Medicine , Medical Society of Virginia , Society for Maternal-Fetal Medicine Disclosure: Nothing to disclose.
What would you like to print?
- Print this section
- Print the entire contents of
- Print the entire contents of article
- HIV in Pregnancy
- Pulmonary Disease and Pregnancy
- Kidney Disease and Pregnancy
- Vaccinations/Immunizations During Pregnancy
- Shock and Pregnancy
- Anemia and Thrombocytopenia in Pregnancy
- Multifetal Pregnancy
- Is immunotherapy for cancer safe in pregnancy?
- Labetalol, Nifedipine: Outcome on Pregnancy Hypertension
- The Pregnancy Challenges of Women With Chronic Conditions

- Drug Interaction Checker
- Pill Identifier
- Calculators

- 2020/viewarticle/immunotherapy-cancer-safe-pregnancy-2024a100083dnews news Is immunotherapy for cancer safe in pregnancy?

- 2002261369-overviewDiseases & Conditions Diseases & Conditions Postterm Pregnancy

- Type 2 Diabetes
- Heart Disease
- Digestive Health
- Multiple Sclerosis
- Diet & Nutrition
- Supplements
- Health Insurance
- Public Health
- Patient Rights
- Caregivers & Loved Ones
- End of Life Concerns
- Health News
- Thyroid Test Analyzer
- Doctor Discussion Guides
- Hemoglobin A1c Test Analyzer
- Lipid Test Analyzer
- Complete Blood Count (CBC) Analyzer
- What to Buy
- Editorial Process
- Meet Our Medical Expert Board
What Is Breech?
When a fetus is delivered buttocks or feet first
- Types of Presentation
Risk Factors
Complications.
Breech concerns the position of the fetus before labor . Typically, the fetus comes out headfirst, but in a breech delivery, the buttocks or feet come out first. This type of delivery is risky for both the pregnant person and the fetus.
This article discusses the different types of breech presentations, risk factors that might make a breech presentation more likely, treatment options, and complications associated with a breech delivery.
Verywell / Jessica Olah
Types of Breech Presentation
During the last few weeks of pregnancy, a fetus usually rotates so that the head is positioned downward to come out of the vagina first. This is called the vertex position.
In a breech presentation, the fetus does not turn to lie in the correct position. Instead, the fetus’s buttocks or feet are positioned to come out of the vagina first.
At 28 weeks of gestation, approximately 20% of fetuses are in a breech position. However, the majority of these rotate to the proper vertex position. At full term, around 3%–4% of births are breech.
The different types of breech presentations include:
- Complete : The fetus’s knees are bent, and the buttocks are presenting first.
- Frank : The fetus’s legs are stretched upward toward the head, and the buttocks are presenting first.
- Footling : The fetus’s foot is showing first.
Signs of Breech
There are no specific symptoms associated with a breech presentation.
Diagnosing breech before the last few weeks of pregnancy is not helpful, since the fetus is likely to turn to the proper vertex position before 35 weeks gestation.
A healthcare provider may be able to tell which direction the fetus is facing by touching a pregnant person’s abdomen. However, an ultrasound examination is the best way to determine how the fetus is lying in the uterus.
Most breech presentations are not related to any specific risk factor. However, certain circumstances can increase the risk for breech presentation.
These can include:
- Previous pregnancies
- Multiple fetuses in the uterus
- An abnormally shaped uterus
- Uterine fibroids , which are noncancerous growths of the uterus that usually appear during the childbearing years
- Placenta previa, a condition in which the placenta covers the opening to the uterus
- Preterm labor or prematurity of the fetus
- Too much or too little amniotic fluid (the liquid that surrounds the fetus during pregnancy)
- Fetal congenital abnormalities
Most fetuses that are breech are born by cesarean delivery (cesarean section or C-section), a surgical procedure in which the baby is born through an incision in the pregnant person’s abdomen.
In rare instances, a healthcare provider may plan a vaginal birth of a breech fetus. However, there are more risks associated with this type of delivery than there are with cesarean delivery.
Before cesarean delivery, a healthcare provider might utilize the external cephalic version (ECV) procedure to turn the fetus so that the head is down and in the vertex position. This procedure involves pushing on the pregnant person’s belly to turn the fetus while viewing the maneuvers on an ultrasound. This can be an uncomfortable procedure, and it is usually done around 37 weeks gestation.
ECV reduces the risks associated with having a cesarean delivery. It is successful approximately 40%–60% of the time. The procedure cannot be done once a pregnant person is in active labor.
Complications related to ECV are low and include the placenta tearing away from the uterine lining, changes in the fetus’s heart rate, and preterm labor.
ECV is usually not recommended if the:
- Pregnant person is carrying more than one fetus
- Placenta is in the wrong place
- Healthcare provider has concerns about the health of the fetus
- Pregnant person has specific abnormalities of the reproductive system
Recommendations for Previous C-Sections
The American College of Obstetricians and Gynecologists (ACOG) says that ECV can be considered if a person has had a previous cesarean delivery.
During a breech delivery, the umbilical cord might come out first and be pinched by the exiting fetus. This is called cord prolapse and puts the fetus at risk for decreased oxygen and blood flow. There’s also a risk that the fetus’s head or shoulders will get stuck inside the mother’s pelvis, leading to suffocation.
Complications associated with cesarean delivery include infection, bleeding, injury to other internal organs, and problems with future pregnancies.
A healthcare provider needs to weigh the risks and benefits of ECV, delivering a breech fetus vaginally, and cesarean delivery.
In a breech delivery, the fetus comes out buttocks or feet first rather than headfirst (vertex), the preferred and usual method. This type of delivery can be more dangerous than a vertex delivery and lead to complications. If your baby is in breech, your healthcare provider will likely recommend a C-section.
A Word From Verywell
Knowing that your baby is in the wrong position and that you may be facing a breech delivery can be extremely stressful. However, most fetuses turn to have their head down before a person goes into labor. It is not a cause for concern if your fetus is breech before 36 weeks. It is common for the fetus to move around in many different positions before that time.
At the end of your pregnancy, if your fetus is in a breech position, your healthcare provider can perform maneuvers to turn the fetus around. If these maneuvers are unsuccessful or not appropriate for your situation, cesarean delivery is most often recommended. Discussing all of these options in advance can help you feel prepared should you be faced with a breech delivery.
American College of Obstetricians and Gynecologists. If your baby is breech .
TeachMeObGyn. Breech presentation .
MedlinePlus. Breech birth .
Hofmeyr GJ, Kulier R, West HM. External cephalic version for breech presentation at term . Cochrane Database Syst Rev . 2015 Apr 1;2015(4):CD000083. doi:10.1002/14651858.CD000083.pub3
By Christine Zink, MD Dr. Zink is a board-certified emergency medicine physician with expertise in the wilderness and global medicine.
- Pregnancy Classes

Breech Births
In the last weeks of pregnancy, a baby usually moves so his or her head is positioned to come out of the vagina first during birth. This is called a vertex presentation. A breech presentation occurs when the baby’s buttocks, feet, or both are positioned to come out first during birth. This happens in 3–4% of full-term births.
What are the different types of breech birth presentations?
- Complete breech: Here, the buttocks are pointing downward with the legs folded at the knees and feet near the buttocks.
- Frank breech: In this position, the baby’s buttocks are aimed at the birth canal with its legs sticking straight up in front of his or her body and the feet near the head.
- Footling breech: In this position, one or both of the baby’s feet point downward and will deliver before the rest of the body.
What causes a breech presentation?
The causes of breech presentations are not fully understood. However, the data show that breech birth is more common when:
- You have been pregnant before
- In pregnancies of multiples
- When there is a history of premature delivery
- When the uterus has too much or too little amniotic fluid
- When there is an abnormally shaped uterus or a uterus with abnormal growths, such as fibroids
- The placenta covers all or part of the opening of the uterus placenta previa
How is a breech presentation diagnosed?
A few weeks prior to the due date, the health care provider will place her hands on the mother’s lower abdomen to locate the baby’s head, back, and buttocks. If it appears that the baby might be in a breech position, they can use ultrasound or pelvic exam to confirm the position. Special x-rays can also be used to determine the baby’s position and the size of the pelvis to determine if a vaginal delivery of a breech baby can be safely attempted.
Can a breech presentation mean something is wrong?
Even though most breech babies are born healthy, there is a slightly elevated risk for certain problems. Birth defects are slightly more common in breech babies and the defect might be the reason that the baby failed to move into the right position prior to delivery.
Can a breech presentation be changed?
It is preferable to try to turn a breech baby between the 32nd and 37th weeks of pregnancy . The methods of turning a baby will vary and the success rate for each method can also vary. It is best to discuss the options with the health care provider to see which method she recommends.
Medical Techniques
External Cephalic Version (EVC) is a non-surgical technique to move the baby in the uterus. In this procedure, a medication is given to help relax the uterus. There might also be the use of an ultrasound to determine the position of the baby, the location of the placenta and the amount of amniotic fluid in the uterus.
Gentle pushing on the lower abdomen can turn the baby into the head-down position. Throughout the external version the baby’s heartbeat will be closely monitored so that if a problem develops, the health care provider will immediately stop the procedure. ECV usually is done near a delivery room so if a problem occurs, a cesarean delivery can be performed quickly. The external version has a high success rate and can be considered if you have had a previous cesarean delivery.
ECV will not be tried if:
- You are carrying more than one fetus
- There are concerns about the health of the fetus
- You have certain abnormalities of the reproductive system
- The placenta is in the wrong place
- The placenta has come away from the wall of the uterus ( placental abruption )
Complications of EVC include:
- Prelabor rupture of membranes
- Changes in the fetus’s heart rate
- Placental abruption
- Preterm labor
Vaginal delivery versus cesarean for breech birth?
Most health care providers do not believe in attempting a vaginal delivery for a breech position. However, some will delay making a final decision until the woman is in labor. The following conditions are considered necessary in order to attempt a vaginal birth:
- The baby is full-term and in the frank breech presentation
- The baby does not show signs of distress while its heart rate is closely monitored.
- The process of labor is smooth and steady with the cervix widening as the baby descends.
- The health care provider estimates that the baby is not too big or the mother’s pelvis too narrow for the baby to pass safely through the birth canal.
- Anesthesia is available and a cesarean delivery possible on short notice
What are the risks and complications of a vaginal delivery?
In a breech birth, the baby’s head is the last part of its body to emerge making it more difficult to ease it through the birth canal. Sometimes forceps are used to guide the baby’s head out of the birth canal. Another potential problem is cord prolapse . In this situation the umbilical cord is squeezed as the baby moves toward the birth canal, thus slowing the baby’s supply of oxygen and blood. In a vaginal breech delivery, electronic fetal monitoring will be used to monitor the baby’s heartbeat throughout the course of labor. Cesarean delivery may be an option if signs develop that the baby may be in distress.
When is a cesarean delivery used with a breech presentation?
Most health care providers recommend a cesarean delivery for all babies in a breech position, especially babies that are premature. Since premature babies are small and more fragile, and because the head of a premature baby is relatively larger in proportion to its body, the baby is unlikely to stretch the cervix as much as a full-term baby. This means that there might be less room for the head to emerge.
Want to Know More?
- Creating Your Birth Plan
- Labor & Birth Terms to Know
- Cesarean Birth After Care
Compiled using information from the following sources:
- ACOG: If Your Baby is Breech
- William’s Obstetrics Twenty-Second Ed. Cunningham, F. Gary, et al, Ch. 24.
- Danforth’s Obstetrics and Gynecology Ninth Ed. Scott, James R., et al, Ch. 21.
BLOG CATEGORIES
- Pregnancy Symptoms 5
- Can I get pregnant if… ? 3
- Paternity Tests 2
- The Bumpy Truth Blog 7
- Multiple Births 10
- Pregnancy Complications 68
- Pregnancy Concerns 62
- Cord Blood 4
- Pregnancy Supplements & Medications 14
- Pregnancy Products & Tests 8
- Changes In Your Body 5
- Health & Nutrition 2
- Labor and Birth 65
- Planning and Preparing 24
- Breastfeeding 29
- Week by Week Newsletter 40
- Is it Safe While Pregnant 55
- The First Year 41
- Genetic Disorders & Birth Defects 17
- Pregnancy Health and Wellness 149
- Your Developing Baby 16
- Options for Unplanned Pregnancy 18
- Child Adoption 19
- Fertility 54
- Pregnancy Loss 11
- Uncategorized 4
- Women's Health 34
- Prenatal Testing 16
- Abstinence 3
- Birth Control Pills, Patches & Devices 21
- Thank You for Your Donation
- Unplanned Pregnancy
- Getting Pregnant
- Healthy Pregnancy
- Privacy Policy
- Pregnancy Questions Center
Share this post:
Similar post.

Episiotomy: Advantages & Complications

Retained Placenta

What is Dilation in Pregnancy?
Track your baby’s development, subscribe to our week-by-week pregnancy newsletter.
- The Bumpy Truth Blog
- Fertility Products Resource Guide
Pregnancy Tools
- Ovulation Calendar
- Baby Names Directory
- Pregnancy Due Date Calculator
- Pregnancy Quiz
Pregnancy Journeys
- Partner With Us
- Corporate Sponsors
6.1 Breech presentation
Presentation of the feet or buttocks of the foetus.
6.1.1 The different breech presentations
- In a complete breech presentation, the legs are tucked, and the foetus is in a crouching position (Figure 6.1a).
- In a frank breech presentation, the legs are extended, raised in front of the torso, with the feet near the head (Figure 6.1b).
- In a footling breech presentation (rare), one or both feet present first, with the buttocks higher up and the lower limbs extended or half-bent (Figure 6.1c).
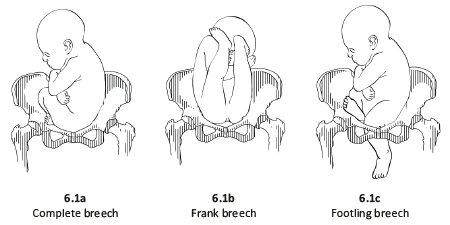
6.1.2 Diagnosis
- The cephalic pole is palpable in the uterine fundus; round, hard, and mobile; the indentation of the neck can be felt.
- The inferior pole is voluminous, irregular, less hard, and less mobile than the head.
- During labour, vaginal examination reveals a “soft mass” divided by the cleft between the buttocks, with a hard projection at end of the cleft (the coccyx and sacrum).
- After rupture of the membranes: the anus can be felt in the middle of the cleft; a foot may also be felt.
- The clinical diagnosis may be difficult: a hand may be mistaken for a foot, a face for a breech.
6.1.3 Management
Route of delivery.
Before labour, external version (Chapter 7, Section 7.7 ) may be attempted to avoid breech delivery.
If external version is contra-indicated or unsuccessful, the breech position alone – in the absence of any other anomaly – is not, strictly speaking, a dystocic presentation, and does not automatically require a caesarean section. Deliver vaginally, if possible – even if the woman is primiparous.
Breech deliveries must be done in a CEmONC facility, especially for primiparous women.
Favourable factors for vaginal delivery are:
- Frank breech presentation;
- A history of vaginal delivery (whatever the presentation);
- Normally progressing dilation during labour.
The footling breech presentation is a very unfavourable position for vaginal delivery (risk of foot or cord prolapse). In this situation, the route of delivery depends on the number of previous births, the state of the membranes and how far advanced the labour is.
During labour
- Monitor dilation every 2 to 4 hours.
- If contractions are of good quality, dilation is progressing, and the foetal heart rate is regular, an expectant approach is best. Do not rupture the membranes unless dilation stops.
- If the uterine contractions are inadequate, labour can be actively managed with oxytocin.
Note : if the dilation stales, transfer the mother to a CEmONC facility unless already done, to ensure access to surgical facility for potential caesarean section.
At delivery
- Insert an IV line before expulsion starts.
- Consider episiotomy at expulsion. Episiotomy is performed when the perineum is sufficiently distended by the foetus's buttocks.
- Presence of meconium or meconium-stained amniotic fluid is common during breech delivery and is not necessarily a sign of foetal distress.
- The infant delivers unaided , as a result of the mother's pushing, simply supported by the birth attendant who gently holds the infant by the bony parts (hips and sacrum), with no traction. Do not pull on the legs.
Once the umbilicus is out, the rest of the delivery must be completed within 3 minutes, otherwise compression of the cord will deprive the infant of oxygen. Do not touch the infant until the shoulder blades appear to avoid triggering the respiratory reflex before the head is delivered.
- Monitor the position of the infant's back; impede rotation into posterior position.
Figures 6.2 - Breech delivery
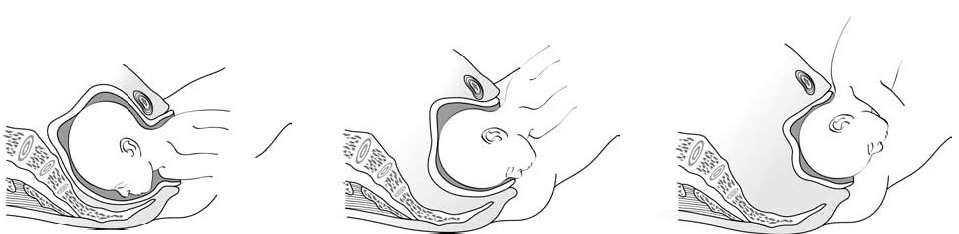
6.1.4 Breech delivery problems
Posterior orientation.
If the infant’s back is posterior during expulsion, take hold of the hips and turn into an anterior position (this is a rare occurrence).
Obstructed shoulders
The shoulders can become stuck and hold back the infant's upper chest and head. This can occur when the arms are raised as the shoulders pass through the mother's pelvis. There are 2 methods for lowering the arms so that the shoulders can descend:
1 - Lovset's manoeuvre
- With thumbs on the infant's sacrum, take hold of the hips and pelvis with the other fingers.
- Turn the infant 90° (back to the left or to the right), to bring the anterior shoulder underneath the symphysis and engage the arm. Deliver the anterior arm.
- Then do a 180° counter-rotation (back to the right or to the left); this engages the posterior arm, which is then delivered.
Figures 6.3 - Lovset's manoeuvre

6.3c - Delivering the anterior arm and shoulder
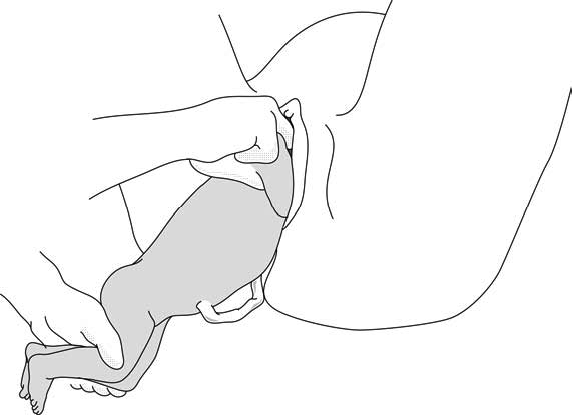
2 - Suzor’s manoeuvre
In case the previous method fails:
- Turn the infant 90° (its back to the right or to the left).
- Pull the infant downward: insert one hand along the back to look for the anterior arm. With the operator thumb in the infant armpit and middle finger along the arm, bring down the arm (Figure 6.4a).
- Lift infant upward by the feet in order to deliver the posterior shoulder (Figure 6.4b).
Figures 6.4 - Suzor's manoeuvre
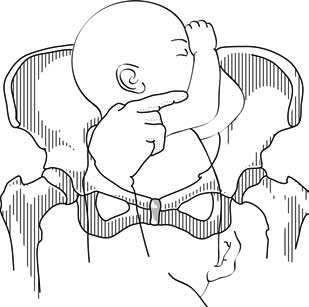
6.4b - Delivering the posterior shoulder
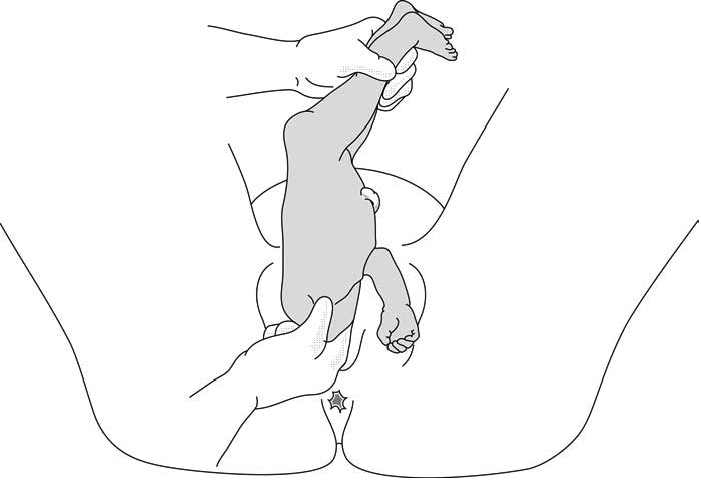
Head entrapment
The infant's head is bulkier than the body, and can get trapped in the mother's pelvis or soft tissue.
There are various manoeuvres for delivering the head by flexing it, so that it descends properly, and then pivoting it up and around the mother's symphysis. These manoeuvres must be done without delay, since the infant must be allowed to breathe as soon as possible. All these manoeuvres must be performed smoothly, without traction on the infant.
1 - Bracht's manoeuvre
- After the arms are delivered, the infant is grasped by the hips and lifted with two hands toward the mother's stomach, without any traction, the neck pivoting around the symphysis.
- Having an assistant apply suprapubic pressure facilitates delivery of the aftercoming head.

2 - Modified Mauriceau manoeuvre
- Infant's head occiput anterior.
- Kneel to get a good traction angle: 45° downward.
- Support the infant on the hand and forearm, then insert the index and middle fingers, placing them on the infant’s maxilla. Placing the index and middle fingers into the infant’s mouth is not recommended, as this can fracture the mandible.
- Place the index and middle fingers of the other hand on either side of the infant's neck and lower the infant's head to bring the sub-occiput under the symphysis (Figure 6.6a).
- Tip the infant’s head and with a sweeping motion bring the back up toward the mother's abdomen, pivoting the occiput around her symphysis pubis (Figure 6.6b).
- Suprapubic pressure on the infant's head along the pelvic axis helps delivery of the head.
- As a last resort, symphysiotomy (Chapter 5, Section 5.7 ) can be combined with this manoeuvre.
Figures 6.6 - Modified Mauriceau manoeuvre
6.6a - Step 1 Infant straddles the birth attendant's forearm; the head, occiput anterior, is lowered to bring the occiput in contact with the symphysis.

6.6b - Step 2 The infant's back is tipped up toward the mother's abdomen.
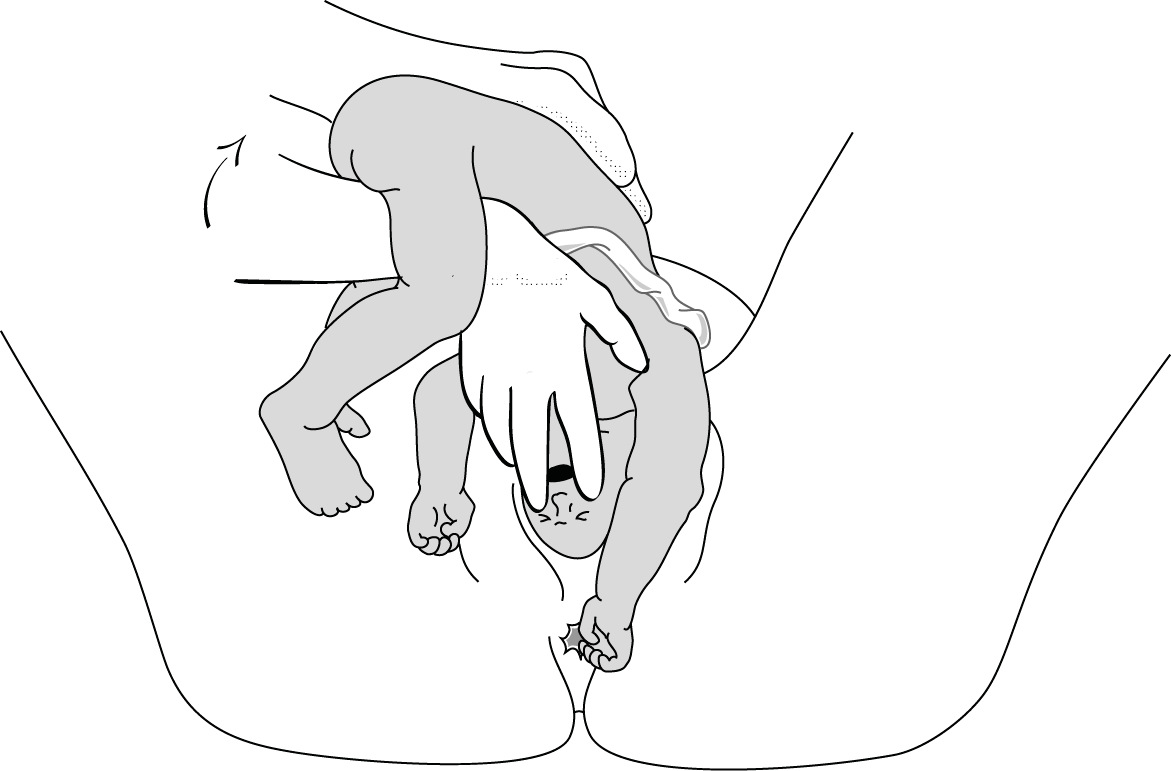
3 - Forceps on aftercoming head
This procedure can only be performed by an operator experienced in using forceps.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
Management of Breech Presentation: A Comparison of Four National Evidence-Based Guidelines
Affiliation.
- 1 Third Department of Obstetrics and Gynaecology, Faculty of Medicine, Aristotle University of Thessaloniki, Greece.
- PMID: 31167240
- DOI: 10.1055/s-0039-1692391
Objective: The management of breech presentation may improve perinatal outcomes. The aim of this study was to synthesize and compare published evidence of four national guidelines on breech presentation.
Study design: A descriptive review of four recently published national guidelines on breech presentation and external cephalic version (ECV) was conducted: Royal College of Obstetricians and Gynaecologists guideline on "External Cephalic Version and Reducing the Incidence of Term Breech Presentation" and "Management of Breech Presentation", American College of Obstetricians and Gynecologists guideline on "External Cephalic Version" and "Mode of Term Singleton Breech Delivery," Society of Obstetricians and Gynaecologists of Canada guideline on "Vaginal Delivery of Breech Presentation" and the Royal Australian and New Zealand College of Obstetricians and Gynaecologists guideline on "Management of breech presentation at term."
Results: Regarding ECV, there is no recommendation by the SOGC, whereas all other national guidelines recommend this technique. Regarding breech vaginal delivery, there are limited recommendations by the ACOG, whereas all other guidelines provide similar recommendations. The RANZCOG makes no special recommendations on the intrapartum period.
Conclusion: The differences among national guidelines point out the need for the adoption of an international consensus on the management of breech presentation.
Thieme. All rights reserved.
PubMed Disclaimer
Conflict of interest statement
None declared.
Similar articles
- Reconsideration of planned vaginal breech delivery in selected cases. Achanna S, Nanda J, Paramjothi P. Achanna S, et al. Med J Malaysia. 2021 May;76(3):390-394. Med J Malaysia. 2021. PMID: 34031339
- Vaginal delivery of breech presentation. Kotaska A, Menticoglou S, Gagnon R; MATERNAL FETAL MEDICINE COMMITTEE. Kotaska A, et al. J Obstet Gynaecol Can. 2009 Jun;31(6):557-566. doi: 10.1016/S1701-2163(16)34221-9. J Obstet Gynaecol Can. 2009. PMID: 19646324 English, French.
- Breech presentation: Clinical practice guidelines from the French College of Gynaecologists and Obstetricians (CNGOF). Sentilhes L, Schmitz T, Azria E, Gallot D, Ducarme G, Korb D, Mattuizzi A, Parant O, Sananès N, Baumann S, Rozenberg P, Sénat MV, Verspyck E. Sentilhes L, et al. Eur J Obstet Gynecol Reprod Biol. 2020 Sep;252:599-604. doi: 10.1016/j.ejogrb.2020.03.033. Epub 2020 Mar 25. Eur J Obstet Gynecol Reprod Biol. 2020. PMID: 32249011 Review.
- Use of external cephalic version for breech pregnancy and mode of delivery for breech and twin pregnancy: a survey of Canadian practitioners. Hutton EK, Hannah ME, Barrett J. Hutton EK, et al. J Obstet Gynaecol Can. 2002 Oct;24(10):804-10. doi: 10.1016/s1701-2163(16)30473-x. J Obstet Gynaecol Can. 2002. PMID: 12399807
- [Breech Presentation: CNGOF Guidelines for Clinical Practice - External Cephalic Version and other Interventions to turn Breech Babies to Cephalic Presentation]. Ducarme G. Ducarme G. Gynecol Obstet Fertil Senol. 2020 Jan;48(1):81-94. doi: 10.1016/j.gofs.2019.10.024. Epub 2019 Oct 31. Gynecol Obstet Fertil Senol. 2020. PMID: 31678503 Review. French.
- Does overweight and obesity have an impact on delivery mode and peripartum outcome in breech presentation? A FRABAT cohort study. Jennewein L, Agel L, Hoock SC, Hentrich AE, Louwen F, Zander N. Jennewein L, et al. Arch Gynecol Obstet. 2024 Jul;310(1):285-292. doi: 10.1007/s00404-024-07403-7. Epub 2024 Mar 18. Arch Gynecol Obstet. 2024. PMID: 38498162 Free PMC article.
- Cephalic version by moxibustion for breech presentation. Coyle ME, Smith C, Peat B. Coyle ME, et al. Cochrane Database Syst Rev. 2023 May 9;5(5):CD003928. doi: 10.1002/14651858.CD003928.pub4. Cochrane Database Syst Rev. 2023. PMID: 37158339 Free PMC article. Review.
- Combined Assessment of the Obstetrical Conjugate and Fetal Birth Weight Predicts Birth Mode Outcome in Vaginally Intended Breech Deliveries of Primiparous Women-A Frabat Study. Zander N, Raimann FJ, Al Naimi A, Brüggmann D, Louwen F, Jennewein L. Zander N, et al. J Clin Med. 2022 Jun 3;11(11):3201. doi: 10.3390/jcm11113201. J Clin Med. 2022. PMID: 35683588 Free PMC article.
- Learning Breech Birth in an Upright Position Is Influenced by Preexisting Experience-A FRABAT Prospective Cohort Study. Jennewein L, Brüggmann D, Fischer K, Raimann FJ, Pfeifenberger HR, Agel L, Zander N, Eichbaum C, Louwen F. Jennewein L, et al. J Clin Med. 2021 May 14;10(10):2117. doi: 10.3390/jcm10102117. J Clin Med. 2021. PMID: 34068873 Free PMC article.
- The influence of the fetal leg position on the outcome in vaginally intended deliveries out of breech presentation at term - A FRABAT prospective cohort study. Jennewein L, Allert R, Möllmann CJ, Paul B, Kielland-Kaisen U, Raimann FJ, Brüggmann D, Louwen F. Jennewein L, et al. PLoS One. 2019 Dec 2;14(12):e0225546. doi: 10.1371/journal.pone.0225546. eCollection 2019. PLoS One. 2019. PMID: 31790449 Free PMC article.
Publication types
- Search in MeSH
Related information
Linkout - more resources, full text sources.
- Georg Thieme Verlag Stuttgart, New York
- Ovid Technologies, Inc.
- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
- Student Success
- Faculty / Staff
- Signature areas
- Faculty Research Expertise
- Funding highlights
- Projects, programs and laboratories
- College Research Centers
- Cultivating Interdisciplinary Research
- Graduate students
- Healthy Discoveries
- Finding a faculty mentor
- Research Support Team
- Preparation
- Request assistance
- Faculty Forums and Workshops
Maternal and neonatal outcomes associated with breech presentation in planned community (home and birth center) births in the United States: A prospective observational cohort study
This research is important because it provides clear evidence about the risks associated with breech births in out-of-hospital settings. This information can help pregnant individuals and healthcare providers make more informed decisions about birth plans when a baby is in a breech position.
College of Health researcher(s)
College unit(s).
Investigate maternal and neonatal outcomes associated with breech presentation in planned community births in the United States, including outcomes associated with types of breech presentation (i.e., frank, complete, footling/kneeling)
Secondary analysis of prospective cohort data from a national perinatal data registry (MANA Stats)
Planned community birth (homes and birth centers), United States
Individuals with a term, singleton gestation (N = 71,943) planning community birth at labor onset
Descriptive statistics to calculate associations between types of breech presentation and maternal and neonatal outcomes
Main outcome measures
Maternal: intrapartum/postpartum transfer, hospitalization, cesarean, hemorrhage, severe perineal laceration, duration of labor stages and membrane rupture
Neonatal: transfer, hospitalization, NICU admission, congenital anomalies, umbilical cord prolapse, birth injury, intrapartum/neonatal death
One percent (n = 695) of individuals experienced breech birth (n = 401, 57.6% vaginally). Most fetuses presented frank breech (57%), with 19% complete, 18% footling/kneeling, and 5% unknown type of breech presentation. Among all breech labors, there were high rates of intrapartum transfer and cesarean birth compared to cephalic presentation (OR 9.0, 95% CI 7.7–10.4 and OR 18.6, 95% CI 15.9–21.7, respectively), with no substantive difference based on parity, planned site of birth, or level of care integration into the health system. For all types of breech presentations, there was increased risk for nearly all assessed neonatal outcomes including hospital transfer, NICU admission, birth injury, and umbilical cord prolapse. Breech presentation was also associated with increased risk of intrapartum/neonatal death (OR 8.5, 95% CI 4.4–16.3), even after congenital anomalies were excluded.
Conclusions
All types of breech presentations in community birth settings are associated with increased risk of adverse neonatal outcomes. These research findings contribute to informed decision-making and reinforce the need for breech training and research and an increase in accessible, high-quality care for planned vaginal breech birth in US hospitals.
- DOI: 10.1016/j.jogoh.2024.102827
- Corpus ID: 271386712
Neonatal outcomes of planned vaginal delivery versus planned cesarean section for breech presentation at term: population-based study on 546,842 breech births across the United States between 2008 and 2017.
- Magdalena Peeva , Nicholas Czuzoj-Shulman , H. Abenhaim
- Published in Journal of Gynecology… 1 July 2024
37 References
Is planned vaginal delivery for breech presentation at term still an option results of an observational prospective survey in france and belgium., outcomes of children at 2 years after planned cesarean birth versus planned vaginal birth for breech presentation at term: the international randomized term breech trial., planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial, vaginal versus cesarean delivery for breech presentation in california: a population‐based study, planned vaginal delivery versus elective caesarean section in singleton term breech presentation: a study of 1116 cases., delivery of breech presentation at term gestation in canada, 2003–2011, singleton vaginal breech delivery at term: still a safe option, outcomes associated with cesarean section versus vaginal breech delivery at a university hospital, cesarean vs. vaginal birth for term breech presentation in 2 different study periods, no. 384-management of breech presentation at term., related papers.
Showing 1 through 3 of 0 Related Papers
- Security analytics and automation

Be prepared for breach disclosure and a magnitude assessment
Organizations need to take a proactive approach to monitoring data stores continuously, and in the case of a breach, assess the magnitude quickly and accurately. dspm can help you..

- Todd Thiemann, Enterprise Strategy Group
We provide market insights, research and advisory, and technical validations for tech buyers.
Updated Securities and Exchange Commission rules that require rapid breach disclosure are causing heartburn for some enterprises and bring to mind the Boy Scouts' "Be prepared" motto. Knowing where your data stores are located and what sensitive data is inside them is fundamental to data security . And in the case of a breach, it's integral to promptly analyze and understand the magnitude of it.
Organizations need a proactive approach to monitoring their data continuously. Data repositories crop up and evolve over time as new applications and services are rolled out. A data store initially created without sensitive data might subsequently have data added. And some individuals might take the initiative to create data without IT and IT security having visibility into that data. Having an accurate understanding of your data assets helps mitigate cybersecurity risk, meet compliance obligations and control the damage if something happens.
SEC breach disclosure rules
The Securities and Exchange Commission (SEC) announced revised rules for disclosing material cybersecurity incidents in June 2023. Those rules require mandatory reporting of material incidents within four business days of determining materiality. Every company has a different equation when it comes to gauging materiality because every business is different. You need to understand what compromised data you are dealing with to help inform that materiality determination. And you need to know which data stores were affected and what is inside them. That is where data discovery and classification come into play.
Data discovery and classification tools might be homegrown, meaning developed internally, or commercial off-the-shelf offerings. Tools run the gamut from backup and restore tools for data protection, data loss prevention tools, cloud access security brokers and data governance tools. When it comes to large data repositories in the cloud or on premises that might have data with more scale and variety, enterprises typically gravitate toward data security posture management (DSPM) tools.
Whatever your approach, being prepared by understanding where your sensitive data stores are located and categorizing the data inside of them will enable you to quickly evaluate the magnitude of a potential breach so you can make an accurate determination of materiality. While reporting a data breach will result in negative PR and reputational damage, accurately determining the magnitude of a breach helps you avoid having to publish multiple notifications to publicly revise the number and type of compromised records.
Overestimating the magnitude of a breach: Marriott International
The hospitality conglomerate Marriott International reported in November 2018 that hackers had breached its Starwood reservation systems and stolen the personal data of up to 500 million guests. The breach affected customers who had reservations with Marriott-owned Starwood properties, such as Sheraton, Westin, W Hotels and St. Regis. The breach started in 2014 and went unnoticed by Starwood for four years. Then, in January 2019, Marriott International subsequently reported the breach had affected 383 million records -- duplicates reduced the number -- and disclosed the breached data included 5 million unencrypted passport numbers, something it had not previously disclosed.
Underestimating the magnitude of a breach: MarineMax
Yacht retailer MarineMax reported a cybersecurity incident to the SEC on March 12, 2024 , for an incident that occurred earlier the month. The company indicated it did not maintain sensitive data in the environment affected by the breach. Then, on April 1, MarineMax amended its SEC filing to indicate financial and personally identifiable information ( PII ) data had been compromised and reported that data affecting more than 123,000 customers and employees had been exposed during the cyberattack. The promptness of this disclosure could be due to the new SEC rule, which was already in effect.
In the case of Marriott International, the initial breach record count was reduced, but the company subsequently disclosed that passport numbers were included in the breached data. In the case of MarineMax, the company initially thought no sensitive data was compromised but subsequently had to disclose that financial data and PII for more than 100,000 people was compromised. The way these cases played out, both companies had to make multiple disclosures over time.
While I have no inside knowledge of either breach, my observation is that quickly conducting the most accurate inventory of where your sensitive data is located and what types of sensitive data are inside your data stores can minimize the reputational damage and compliance risk resulting from a breach.
Data discovery and classification dynamics
In the heat of the moment in a data breach, analysis and reporting missteps can happen. The consequences of not knowing where your data is located and what it contains makes a bad situation even worse when analyzing and reporting on the breach.
While you might have an internally developed tool to identify your data stores and categorize the data inside, the tool can be brittle and miss sensitive data. Internal tools frequently don't locate shadow data outside the control and oversight of IT and IT security teams. Maintaining a homegrown tool can also divert scarce resources from more impactful projects.
DSPM technologies are relatively new and are designed to discover, classify and monitor data stores at scale. Constituents I have spoken with typically uncover previously undiscovered sensitive data when they test a DSPM tool and compare it to their existing, homegrown or legacy tool for data discovery and classification.
While DSPM technology can help to accurately assess the magnitude of a breach, its major value is to help prevent a breach in the first place -- the posture management in data security posture management. Such tools also contribute to improving data governance and regulatory compliance . Understanding what sensitive data you have, where it is located and who is accessing it enables you to take action to mitigate risk and better secure the data. Remediation actions can take many forms, from encrypting or masking the data to revoking outdated access to sensitive data to decommissioning unneeded or deprecated data.
Getting ahead of the problem: Locate and categorize sensitive data stores
You can't secure and report on something you don't know exists. In the same way you might scan a network to understand what devices exist and their security posture, you need to scan for sensitive data repositories and understand what is inside of them.
Your data is dynamic. Lines of business and staff create, update or combine existing data stores. Some of this might be sanctioned, with IT having visibility to the data store; however, some might be unsanctioned, with someone taking the initiative to use data without the IT and IT security team having visibility to the new repository -- the shadow data problem. This data is ever changing and moving, and it requires continually rediscovering and reclassifying sensitive data across your environment, both on premises and in the cloud. Accommodating this data dynamism is where DSPM products shine and homegrown options frequently stumble. As I learned in scouting, the bottom line is to be prepared. Locating your sensitive data stores and categorizing the data inside them on an ongoing basis will enable you to better secure that data, recover it in the event of a ransomware attack and recover more quickly should a breach occur.
Todd Thiemann is a senior analyst covering Identity Access Management (IAM) & Data Security for TechTarget's Enterprise Research Group. He has more than 20 years of experience in cybersecurity marketing and strategy.
Enterprise Strategy Group is a division of TechTarget. Its analysts have business relationships with technology vendors.
Dig Deeper on Security analytics and automation

Top 6 data security posture management use cases
Laminar security posture tech now part of Rubrik platform

6 data security predictions for 2023

How data security posture management complements CSPM
Wi-Fi 6 was introduced as the next-generation Wi-Fi standard after Wi-Fi 5. While similar in certain aspects, Wi-Fi 5 and Wi-Fi 6...
Networks differ based on size, connectivity, coverage and design. This guide explores the most common types of networks, their ...
NaaS, with its varied definitions and attributes, is hard to define. In a new EMA survey, enterprises laid out their expectations...
Enterprises can scale generative AI deployments in different ways. Each alternative comes with its own set of cost considerations...
From consumers to employees to investors, more people are choosing companies that prioritize environmental, social and governance...
As the FTC noncompete ban faces legal challenges, some in Congress including Sen. Elizabeth Warren are supporting the FTC's ...
Enterprises with the IT talent might turn to open-source software as a backup for commercial products to mitigate damage from a ...
Copilot is a powerful generative AI technology with lots of integrations with Microsoft technology. But the usefulness of this ...
The copyright laws around generative AI-created content are still somewhat unclear, so organizations should look to Microsoft's ...
Are you ready for the newest version of the CompTIA Cloud+ exam? Learn exam prep tips from the author of The Official CompTIA ...
While it's tough to make a clear distinction between cloud-native, cloud-based and cloud-enabled apps, they differ in terms of ...
Receiving a FinOps certification helps individuals develop their cloud financial management skills. Discover training and ...
Global comms tech provider enters into collaboration with digital transformation services consultancy to deploy Network as Code ...
With Labour returning to 10 Downing Street after 14 years, the Computer Weekly Security Think Tank panellists share advice and ...
Government scraps £1.3bn worth of AI and tech programmes launched by the Conservatives, but says it is committed to building ...
Mobile Menu Overlay
The White House 1600 Pennsylvania Ave NW Washington, DC 20500
FACT SHEET: Biden- Harris Administration Announces New AI Actions and Receives Additional Major Voluntary Commitment on AI
Nine months ago, President Biden issued a landmark Executive Order to ensure that America leads the way in seizing the promise and managing the risks of artificial intelligence (AI). This Executive Order built on the voluntary commitments he and Vice President Harris received from 15 leading U.S. AI companies last year. Today, the administration announced that Apple has signed onto the voluntary commitments, further cementing these commitments as cornerstones of responsible AI innovation. In addition, federal agencies reported that they completed all of the 270-day actions in the Executive Order on schedule, following their on-time completion of every other task required to date . Agencies also progressed on other work directed for longer timeframes. Following the Executive Order and a series of calls to action made by Vice President Harris as part of her major policy speech before the Global Summit on AI Safety, agencies all across government have acted boldly. They have taken steps to mitigate AI’s safety and security risks, protect Americans’ privacy, advance equity and civil rights, stand up for consumers and workers, promote innovation and competition, advance American leadership around the world, and more. Actions that agencies reported today as complete include the following: Managing Risks to Safety and Security: Over 270 days, the Executive Order directed agencies to take sweeping action to address AI’s safety and security risks, including by releasing vital safety guidance and building capacity to test and evaluate AI. To protect safety and security, agencies have:
- Released for public comment new technical guidelines from the AI Safety Institute (AISI) for leading AI developers in managing the evaluation of misuse of dual-use foundation models. AISI’s guidelines detail how leading AI developers can help prevent increasingly capable AI systems from being misused to harm individuals, public safety, and national security, as well as how developers can increase transparency about their products.
- Published final frameworks on managing generative AI risks and securely developing generative AI systems and dual-use foundation models. These documents by the National Institute of Standards and Technology (NIST) will provide additional guidance that builds on NIST’s AI Risk Management Framework, which offered individuals, organizations, and society a framework to manage AI risks and has been widely adopted both in the U.S. and globally. NIST also submitted a report to the White House outlining tools and techniques to reduce the risks from synthetic content.
- Developed and expanded AI testbeds and model evaluation tools at the Department of Energy (DOE). DOE, in coordination with interagency partners, is using its testbeds to evaluate AI model safety and security, especially for risks that AI models might pose to critical infrastructure, energy security, and national security. DOE’s testbeds are also being used to explore novel AI hardware and software systems, including privacy-enhancing technologies that improve AI trustworthiness. The National Science Foundation (NSF) also launched an initiative to help fund researchers outside the federal government design and plan AI-ready testbeds.
- Reported results of piloting AI to protect vital government software. The Department of Defense (DoD) and Department of Homeland Security (DHS) reported findings from their AI pilots to address vulnerabilities in government networks used, respectively, for national security purposes and for civilian government. These steps build on previous work to advance such pilots within 180 days of the Executive Order.
- Issued a call to action from the Gender Policy Council and Office of Science and Technology Policy to combat image-based sexual abuse, including synthetic content generated by AI. Image-based sexual abuse has emerged as one of the fastest growing harmful uses of AI to-date, and the call to action invites technology companies and other industry stakeholders to curb it. This call flowed from Vice President Harris’s remarks in London before the AI Safety Summit, which underscored that deepfake image-based sexual abuse is an urgent threat that demands global action.
Bringing AI Talent into Government Last year, the Executive Order launched a government-wide AI Talent Surge that is bringing hundreds of AI and AI-enabling professionals into government. Hired individuals are working on critical AI missions, such as informing efforts to use AI for permitting, advising on AI investments across the federal government, and writing policy for the use of AI in government.
- To increase AI capacity across the federal government for both national security and non-national security missions, the AI Talent Surge has made over 200 hires to-date, including through the Presidential Innovation Fellows AI cohort and the DHS AI Corps .
- Building on the AI Talent Surge 6-month report , the White House Office of Science and Technology Policy announced new commitments from across the technology ecosystem, including nearly $100 million in funding, to bolster the broader public interest technology ecosystem and build infrastructure for bringing technologists into government service.
Advancing Responsible AI Innovation President Biden’s Executive Order directed further actions to seize AI’s promise and deepen the U.S. lead in AI innovation while ensuring AI’s responsible development and use across our economy and society. Within 270 days, agencies have:
- Prepared and will soon release a report on the potential benefits, risks, and implications of dual-use foundation models for which the model weights are widely available, including related policy recommendations. The Department of Commerce’s report draws on extensive outreach to experts and stakeholders, including hundreds of public comments submitted on this topic.
- Awarded over 80 research teams’ access to computational and other AI resources through the National AI Research Resource (NAIRR) pilot —a national infrastructure led by NSF, in partnership with DOE, NIH, and other governmental and nongovernmental partners, that makes available resources to support the nation’s AI research and education community. Supported projects will tackle deepfake detection, advance AI safety, enable next-generation medical diagnoses and further other critical AI priorities.
- Released a guide for designing safe, secure, and trustworthy AI tools for use in education. The Department of Education’s guide discusses how developers of educational technologies can design AI that benefits students and teachers while advancing equity, civil rights, trust, and transparency. This work builds on the Department’s 2023 report outlining recommendations for the use of AI in teaching and learning.
- Published guidance on evaluating the eligibility of patent claims involving inventions related to AI technology, as well as other emerging technologies. The guidance by the U.S. Patent and Trademark Office will guide those inventing in the AI space to protect their AI inventions and assist patent examiners reviewing applications for patents on AI inventions.
- Issued a report on federal research and development (R&D) to advance trustworthy AI over the past four years. The report by the National Science and Technology Council examines an annual federal AI R&D budget of nearly $3 billion.
- Launched a $23 million initiative to promote the use of privacy-enhancing technologies to solve real-world problems, including related to AI. Working with industry and agency partners, NSF will invest through its new Privacy-preserving Data Sharing in Practice program in efforts to apply, mature, and scale privacy-enhancing technologies for specific use cases and establish testbeds to accelerate their adoption.
- Announced millions of dollars in further investments to advance responsible AI development and use throughout our society. These include $30 million invested through NSF’s Experiential Learning in Emerging and Novel Technologies program—which supports inclusive experiential learning in fields like AI—and $10 million through NSF’s ExpandAI program, which helps build capacity in AI research at minority-serving institutions while fostering the development of a diverse, AI-ready workforce.
Advancing U.S. Leadership Abroad President Biden’s Executive Order emphasized that the United States lead global efforts to unlock AI’s potential and meet its challenges. To advance U.S. leadership on AI, agencies have:
- Issued a comprehensive plan for U.S. engagement on global AI standards. The plan, developed by the NIST, incorporates broad public and private-sector input, identifies objectives and priority areas for AI standards work, and lays out actions for U.S. stakeholders including U.S. agencies. NIST and others agencies will report on priority actions in 180 days.
- Developed guidance for managing risks to human rights posed by AI. The Department of State’s “Risk Management Profile for AI and Human Rights”—developed in close coordination with NIST and the U.S. Agency for International Development—recommends actions based on the NIST AI Risk Management Framework to governments, the private sector, and civil society worldwide, to identify and manage risks to human rights arising from the design, development, deployment, and use of AI.
- Launched a global network of AI Safety Institutes and other government-backed scientific offices to advance AI safety at a technical level. This network will accelerate critical information exchange and drive toward common or compatible safety evaluations and policies.
- Launched a landmark United Nations General Assembly resolution . The unanimously adopted resolution, with more than 100 co-sponsors, lays out a common vision for countries around the world to promote the safe and secure use of AI to address global challenges.
- Expanded global support for the U.S.-led Political Declaration on the Responsible Military Use of Artificial Intelligence and Autonomy. Fifty-five nations now endorse the political declaration, which outlines a set of norms for the responsible development, deployment, and use of military AI capabilities.
The Table below summarizes many of the activities that federal agencies have completed in response to the Executive Order:

Stay Connected
We'll be in touch with the latest information on how President Biden and his administration are working for the American people, as well as ways you can get involved and help our country build back better.
Opt in to send and receive text messages from President Biden.
IMAGES
VIDEO
COMMENTS
Breech presentation refers to the fetus in the longitudinal lie with the buttocks or lower extremity entering the pelvis first. The three types of breech presentation include frank breech, complete breech, and incomplete breech. In a frank breech, the fetus has flexion of both hips, and the legs are straight with the feet near the fetal face, in a pike position.
Breech presentation of the fetus in late pregnancy may result in prolonged or obstructed labour with resulting risks to both woman and fetus. Interventions to correct breech presentation (to cephalic) before labour and birth are important for the woman's and the baby's health. The aim of this review is to determine the most effective way of ...
Management of Breech Presentation. This is the fourth edition of this guideline originally published in 1999 and revised in 2001 and 2006 under the same title. Executive summary of recommendations What information should be given to women with breech presentation at term?
Labour with a preterm breech should be managed as with a term breech. C. Where there is head entrapment, incisions in the cervix (vaginal birth) or vertical uterine D incision extension (caesarean section) may be used, with or without tocolysis. Evidence concerning the management of preterm labour with a breech presentation is lacking.
Breech presentation, which occurs in approximately 3 percent of fetuses at term, describes the fetus whose presenting part is the buttocks and/or feet. Although most breech fetuses have normal anatomy, this presentation is associated with an increased risk for congenital malformations and mild deformations, torticollis, and developmental ...
Breech and external cephalic version. Breech presentation is when the fetus is lying longitudinally and its buttocks, foot or feet are presenting instead of its head. Figure 1. Breech presentations. Breech presentation occurs in three to four per cent of term deliveries and is more common in nulliparous women.
Management of Breech Presentation (Green-top Guideline No. 20b) Summary: The aim of this guideline is to aid decision making regarding the route of delivery and choice of various techniques used during delivery. It does not include antenatal or postnatal care. Information regarding external cephalic version is the topic of the separate Royal ...
Summary. Breech presentation refers to the baby presenting for delivery with the buttocks or feet first rather than head. Associated with increased morbidity and mortality for the mother in terms of emergency cesarean section and placenta previa; and for the baby in terms of preterm birth, small fetal size, congenital anomalies, and perinatal ...
Breech birth is a divisive clinical issue, however vaginal breech births continue to occur despite a globally high caesarean section rate for breech presenting fetuses. Inconsistencies are known to exist between clinical practice guidelines relating to the management of breech presentation.
Breech delivery is the single most common abnormal presentation. The incidence is highly dependent on the gestational age. At 20 weeks, about one in four pregnancies are breech presentation. By full term, the incidence is about 4%. Other contributing factors include: Abnormal shape of the pelvis, uterus, or abdominal wall,
In breech presentation, the presenting part is a poor dilating wedge, which can cause the head to be trapped during delivery, often compressing the umbilical cord. For breech presentation, usually do cesarean delivery at 39 weeks or during labor, but external cephalic version is sometimes successful before labor, usually at 37 or 38 weeks.
The most widely quoted study regarding the management of breech presentation at term is the 'Term Breech Trial'. Published in 2000, this large, international multicenter randomised clinical trial compared a policy of planned vaginal delivery with planned caesarean section for selected breech presentations.
Overview. Breech presentation is defined as a fetus in a longitudinal lie with the buttocks or feet closest to the cervix. This occurs in 3-4% of all deliveries. The percentage of breech deliveries decreases with advancing gestational age from 22-25% of births prior to 28 weeks' gestation to 7-15% of births at 32 weeks' gestation to 3-4% of ...
The management of breech presentation continues to cause academic and clinical contention globally [[1], [2], [3]]. In recent years, research has shown that if certain criteria are met, and appropriately experienced and skilled clinicians are available, Vaginal Breech Birth (VBB) is a safe option [[4], [5], [6]].
To identify the clinical management required for a woman with a breech baby giving birth at a CTMUHB hospital. To encourage individualised care and support for women with a breech presentation, thus improving both the experience and outcome for mother and baby. 2. Definition.
At full term, around 3%-4% of births are breech. The different types of breech presentations include: Complete: The fetus's knees are bent, and the buttocks are presenting first. Frank: The fetus's legs are stretched upward toward the head, and the buttocks are presenting first. Footling: The fetus's foot is showing first.
Breech Births. In the last weeks of pregnancy, a baby usually moves so his or her head is positioned to come out of the vagina first during birth. This is called a vertex presentation. A breech presentation occurs when the baby's buttocks, feet, or both are positioned to come out first during birth. This happens in 3-4% of full-term births.
Management of Breech Presentation Breech presentation refers to a fetal position in which the baby's buttocks or feet are positioned to be delivered first instead of the head. While most babies naturally assume a head-down position for birth, occurring in about 3-4% of pregnancies, breech presentation presents unique challenges and
The debate surrounding the management of term breech presentation has excessively focused on the mode of delivery. Indeed, a steady decline in the rate of vaginal breech delivery has been observed over the last three decades, and the soundness of the vaginal route was seriously challenged at the beginning of the 2000s. However, associations between adverse perinatal outcomes and antenatal risk ...
Breech - Management of. 1. Purpose. This document provides details of clinical management of women who have a diagnosis of breech presentation during pregnancy or intrapartum at the Women's. This procedure outlines the decision and management process required for: breech presentation diagnosed antenatally.
Presentation of the feet or buttocks of the foetus. 6.1.1 The different breech presentations. In a complete breech presentation, the legs are tucked, and the foetus is in a crouching position (Figure 6.1a).; In a frank breech presentation, the legs are extended, raised in front of the torso, with the feet near the head (Figure 6.1b).; In a footling breech presentation (rare), one or both feet ...
Objective: The management of breech presentation may improve perinatal outcomes. The aim of this study was to synthesize and compare published evidence of four national guidelines on breech presentation. Study design: A descriptive review of four recently published national guidelines on breech presentation and external cephalic version (ECV) was conducted: Royal College of Obstetricians and ...
Conclusion. Although the management of breech presentation at birth still remains a dilemma, even in the modern obstetrics, we must point out that national protocols are needed for a better result. For a trial a labor we need special selection criteria, intrapartum management parameters and practiced delivery techniques. Vaginal breech delivery ...
All types of breech presentations in community birth settings are associated with increased risk of adverse neonatal outcomes. These research findings contribute to informed decision-making and reinforce the need for breech training and research and an increase in accessible, high-quality care for planned vaginal breech birth in US hospitals. ...
Semantic Scholar extracted view of "Neonatal outcomes of planned vaginal delivery versus planned cesarean section for breech presentation at term: population-based study on 546,842 breech births across the United States between 2008 and 2017." by Magdalena Peeva et al. ... No. 384-Management of Breech Presentation at Term.
Insurers have begun calculating the financial damage caused by last week's devastating CrowdStrike software glitch that crashed computers, canceled flights and disrupted hospitals all around the ...
While DSPM technology can help to accurately assess the magnitude of a breach, its major value is to help prevent a breach in the first place -- the posture management in data security posture management. Such tools also contribute to improving data governance and regulatory compliance. Understanding what sensitive data you have, where it is ...
The Department of State's "Risk Management Profile for AI and Human Rights"—developed in close coordination with NIST and the U.S. Agency for International Development—recommends actions ...
Action Item 1.3.4: Develop a Basin drought contingency plan for management of supplies during times of shortage. o Basin-wide Drought Contingency Plan to be completed within the first 3 to 5 years of 2 nd increment and address conditions under a basin- wide or regional drought condition. o