
How to Write an Action Plan: Step-by-Step (Examples)
By Status.net Editorial Team on November 9, 2023 — 9 minutes to read
An action plan is a detailed roadmap of the necessary steps you need to take to achieve a specific goal or objective. It’s like a GPS that guides you from your starting point to your desired destination. Creating an action plan helps you break down a large goal into smaller, more manageable tasks, which makes the goal feel less overwhelming.
To start, you should first identify your end goal and be as specific as possible. For example, if you want to increase sales for your business, set a target like “Increase sales by 20% within the next six months.” This will give you a clear vision of what you want to achieve and make it easier to measure your progress.
Next, list the necessary actions or tasks required to reach your goal. These can be further divided into smaller tasks that are easy to understand and implement. For example, to increase sales, you could:
- Improve your online presence by revamping your website, optimizing it for search engines, and posting regularly on social media platforms.
- Reach out to potential clients through email campaigns and cold calls.
- Offer promotions or discounts to incentivize new customers to try your product or service.
Now, it’s time to set a timeline for each task. Deadlines will enable you to monitor your progress and stay on track. Assign realistic due dates for each task, and if needed, break them down into smaller milestones.
To ensure your action plan’s success, make sure to assign responsibility for each task. If you’re working with a team, delegate tasks according to each team member’s strengths, skills, and workload. This will help ensure everyone knows what their responsibilities are, and they are held accountable.
Lastly, always monitor your progress and evaluate your action plan’s effectiveness. Regularly review the tasks you’ve accomplished, and make note of the tasks that were challenging or required more time than anticipated. This self-assessment will help you improve your action plan and make necessary adjustments as you work towards your goal.
Example Action Plan
Goal : Increase sales by 20% within the next 6 months (By January 1st, 2025)
Actions : 1. Improve online presence a) Revamp website design – Due October 15th b) Optimize website for SEO – Due November 1st c) Post regularly on social media (1x/week min) – Ongoing
2. Reach out to potential clients a) Create email marketing campaign – Due September 15th b) Start cold calling campaign (10 calls/day) – Start October 1st
3. Offer promotions a) Design promotion flyers – Due September 1st b) Run month-long 20% off sale – October 1-31st
Monitoring : – Check website analytics weekly – Track new clients monthly – Evaluate sales figures monthly – Adjust plan as needed at monthly meetings
Responsibilities : – John to revamp website – Susan to handle social media – Michael to create promotions – Jennifer to manage outreach campaigns
Steps to Creating a Powerhouse Action Plan
First, identify your goal . Be specific about what you want to achieve and set a time frame for accomplishing it. This will help keep your efforts focused and prevent you from getting overwhelmed by smaller tasks. For example, instead of “increase sales”, choose “increase sales by 20% in the next six months”.
Next, break your goal down into smaller, manageable tasks . Create a list of activities or steps that must be completed in order to reach your goal. If your goal is to Increase sales by 20%, some tasks might be:
- Research your target market
- Develop a marketing strategy
- Improve product offerings
- Train your sales team
Assign a deadline and responsible party for each task on your list. This will help ensure that all tasks are completed on time and that everyone knows their role in achieving the goal. Make sure to set realistic timelines for each task, taking into consideration the resources and time available.
Here’s an example:
- Research your target market – due in one week – assigned to Jane (marketing specialist)
- Develop a marketing strategy – due in two weeks – assigned to marketing team
Monitor your progress regularly. Keep track of your progress by using tools such as calendars, project management software, or a simple spreadsheet. Regularly assess whether you’re on track to meet your goal and adjust your action plan if needed. For example, if a task is taking longer than expected, you may need to reassign resources or revise the deadline.
Celebrate your milestones and learn from setbacks . Along the way, take the time to acknowledge and celebrate your successes, as well as learn from any setbacks or challenges. This will help maintain motivation and encourage continuous improvement.
Finally, communicate your action plan to all stakeholders involved, such as employees, investors, or clients. Clear communication ensures everyone understands the goal, their responsibilities, and the expectations for the project.
Defining Clear and Smart Goals
Specific goals.
When creating your action plan, start by setting specific goals. These are clear, well-defined goals that leave no room for ambiguity. You should know exactly what needs to be accomplished and how you plan to achieve it. For example, instead of aiming for “increasing sales,” set a goal like “increase sales by 15% over the next six months.”
Measurable Goals
Your goals should be measurable so that you can track your progress and know when you’ve achieved them. This involves identifying quantifiable indicators that will help you determine your progress. For instance, if your goal is to increase sales, a measurable component can be the number of units sold or the amount of revenue generated within a specific timeframe.
Achievable Goals
When setting goals, make sure they are achievable and realistic based on your current resources and constraints. Consider your team’s capabilities, time, and budget. Unattainable goals may negatively impact your motivation and morale. For example, if you have a small team with limited resources, setting a goal to double your company’s size within a month might be unrealistic. Instead, aim for a modest yet challenging growth rate that can be achieved with your available resources.
Relevant Goals
Your action plan goals should also be relevant to your organization’s mission and vision. These are goals that align with your overall strategic plan and contribute to its long-term success. Relevant goals ensure that your efforts are focused on high-impact areas and avoid unnecessary distractions. For example, if your business is focused on sustainability, a relevant goal might be to reduce your company’s carbon footprint by 20% in the next year.
Time-bound Goals
Finally, ensure that your goals are time-bound, meaning they have a deadline for completion. Deadlines keep your team accountable and help maintain a sense of urgency, which is crucial for staying on track and achieving your objectives. A clear timeframe also allows you to measure your progress and adjust your plans as needed. For instance, you could set a goal to expand your customer base by 10% within the next quarter.
Assigning Roles and Responsibilities
When creating an action plan, it’s important to assign roles and responsibilities to your team members. This helps ensure tasks are completed efficiently and everyone is clear about their duties. Here’s how to do it effectively:
- First, identify the necessary tasks to achieve your goal. Be specific about what needs to be done and break it down into smaller steps if needed. For example, if your action plan involves promoting a new product, tasks could include designing promotional materials, creating social media posts, and reaching out to potential partners.
- Next, evaluate the skills and expertise of your team members. Consider their strengths, weaknesses, and past experiences with similar projects. This will help you match team members with tasks that best suit their abilities. For instance, someone with graphic design expertise should be responsible for creating promotional materials.
- Once you’ve determined which team members are best suited for each task, clearly communicate their roles and responsibilities. This can be done through a project management tool, an email, or a team meeting. Make sure everyone is aware of their duties and the deadlines for each task.
- Keep track of everyone’s progress, and hold regular check-ins to see how each team member is doing with their assigned tasks.
- Be open to adjusting your action plan and roles as necessary. Sometimes, unforeseen challenges can arise and require you to modify your plan.
Creating a Time Frame
When working on your action plan, it’s important to establish a realistic time frame for achieving your goals. This helps you stay on track and prioritize tasks effectively. We will walk you through the process of creating a time frame for your action plan.
- First, break down your primary goal into smaller, manageable tasks. Think of these tasks as stepping stones that will lead you toward your overall objective. For example, if your goal is to start a new business, your tasks might include researching your target market, establishing a budget, and developing a marketing strategy.
- Next, assign a deadline to each task. Deadlines should be specific and set in stone but make sure to be flexible enough to adjust as necessary. Use a calendar or planner to visualize your timeline, marking important dates and milestones. For example, you could set a four-month deadline for completing market research and a six-month deadline for securing initial funding.
- To keep yourself accountable, set reminders or notifications for important deadlines. This can be done using digital tools like smartphone apps or traditional methods, such as sticky notes on your workspace. Regularly reviewing your progress and adjusting your time frame when needed will help you stay on track.
- Lastly, consider any external factors that might impact your time frame. Are there seasonal events, holidays, or industry-specific deadlines that could affect your ability to complete tasks? Factor in these considerations as you build your timeline.
Resource Allocation
When creating an action plan, resource allocation plays a major role. You’ll need to determine the resources required for each task and how they’ll be distributed among team members. This usually includes time, budget, and human resources.
- Start by estimating the time each task will take. Break tasks down into smaller chunks and allocate a specific deadline to each. This will help you prioritize tasks and balance workloads for your team members. For example, if designing a marketing campaign takes four weeks, divide it into weekly tasks like conducting market research, creating promotional materials, and setting up advertisements.
- Next, determine the budget needed to complete your project. Identify any expenses such as salaries, equipment, software, and project-related costs like travel. Create a budget for each task to avoid overspending, and allocate funds accordingly. Using our marketing campaign example, allocate separate budgets for market research tools, graphic design tools, and advertising platforms.
- Lastly, allocate human resources to tasks based on their skills and expertise. Delegate responsibilities to your team members, ensuring that everyone has a clear understanding of their role in the project. If needed, identify additional hires or outside consultants to fill gaps in your team’s expertise. For instance, if your team lacks graphic design experience, consider hiring a graphic designer or outsourcing the work to a design agency.
- 6 Examples: How to Write a Perfect Proposal Letter (Step-by-Step)
- How to Write a Performance Improvement Plan (PIP)
- 2 Templates and Examples: Individual Development Plan
- How to Write a Perfect Project Plan? [The Easy Guide]
- How to Write Inspiring Core Values? 5 Steps with Examples
- 2 Detailed Examples: How To Write a Professional Email
We use essential cookies to make Venngage work. By clicking “Accept All Cookies”, you agree to the storing of cookies on your device to enhance site navigation, analyze site usage, and assist in our marketing efforts.
Manage Cookies
Cookies and similar technologies collect certain information about how you’re using our website. Some of them are essential, and without them you wouldn’t be able to use Venngage. But others are optional, and you get to choose whether we use them or not.
Strictly Necessary Cookies
These cookies are always on, as they’re essential for making Venngage work, and making it safe. Without these cookies, services you’ve asked for can’t be provided.
Show cookie providers
- Google Login
Functionality Cookies
These cookies help us provide enhanced functionality and personalisation, and remember your settings. They may be set by us or by third party providers.
Performance Cookies
These cookies help us analyze how many people are using Venngage, where they come from and how they're using it. If you opt out of these cookies, we can’t get feedback to make Venngage better for you and all our users.
- Google Analytics
Targeting Cookies
These cookies are set by our advertising partners to track your activity and show you relevant Venngage ads on other sites as you browse the internet.
- Google Tag Manager
- Infographics
- Daily Infographics
- Popular Templates
- Accessibility
- Graphic Design
- Graphs and Charts
- Data Visualization
- Human Resources
- Beginner Guides
Blog Beginner Guides What is an Action Plan & How to Write One [With Examples]
What is an Action Plan & How to Write One [With Examples]
Written by: Danesh Ramuthi Oct 26, 2023

An action plan is a meticulously structured strategy that pinpoints specific steps, tasks and resources vital to turning a goal into reality. It is extremely useful in any project management.
Crafting an action plan is like plotting a route for a cross-country journey. It’s the strategic map that outlines every step, decision and pitstop needed to reach your ultimate destination.
With a well-thought-out action plan, you’re not just shooting in the dark; you’re making informed, purposeful strides towards your goals. Dive deep with our guide and witness real-world examples that will inspire and guide you.
Need a tool to kickstart your planning? Try out the Venngage business plan maker and explore their extensive collection of action plan templates .
Click to jump ahead:
What is the purpose of an action plan?
When to develop an action plan, 7 components of a actions plan, 15 action plan examples.
- How to Write an action plan?
Final thoughts
An action plan serves as a strategic tool designed to outline specific steps, tasks and goals necessary to achieve a particular objective.
Its primary purpose is to provide a clear roadmap and direction for individuals, teams or organizations to follow in order to efficiently and effectively accomplish their goals.
Action plans break down complex projects into manageable, actionable components, making it easier to track progress and stay on course.
Moreover, action plans play a crucial role in fostering accountability and coordination among team members. By assigning responsibilities and deadlines for each task or milestone, they ensure that everyone involved is aware of their roles and the overall timeline, reducing confusion and enhancing teamwork.
Additionally, action plans help in resource allocation, budgeting and risk management by enabling stakeholders to identify potential challenges and plan for contingencies.
Overall, the purpose of an action plan is to transform abstract goals into concrete actions, making them more achievable and measurable while ensuring that the resources and efforts are aligned with the desired outcomes.
Developing an action plan is crucial when you’re looking to achieve a specific goal or outcome. Here are instances when you should consider developing an action plan:
- Start of an organization : Ideally, an action plan should be developed within the first six months to one year of the start of an organization. This initial plan lays the groundwork for the future direction and growth of the entity.
- Project initiation : At the start of any project, an action plan helps to clearly define the tasks, responsibilities, and timelines.
- Goal setting : Whenever you or your organization sets a new goal. Action plans transform these goals from abstract ideas into concrete steps.
- Strategic planning : For long-term visions and missions, action plans break down the journey into manageable pieces, each with its timeline and responsible parties.
- Performance improvement : If there are areas where performance is lacking, whether it’s personal or organizational, an action plan can outline the steps needed to elevate performance.
An action plan is a detailed outline that breaks down the steps necessary to achieve a specific goal. Here are the typical components of an action plan.
1. Objective or Goal
The cornerstone of your action plan is the objective or goal. This should be a clear and concise statement outlining the desired outcome or result. Having a well-defined objective provides a direction and purpose to the entire plan, ensuring all tasks and actions are aligned towards achieving this singular aim.
2. Tasks or Actions
Once the objective is set, the next step is to list down the specific tasks or actions required to achieve this goal. These tasks should be broken down into detailed steps, ensuring no essential activity is overlooked. The granularity of these tasks can vary based on the complexity of the goal.
3. Set deadline
For each task or action, set a realistic and achievable deadline. This timeline ensures that the plan stays on track and that momentum is maintained throughout the execution. It also allows for monitoring progress and identifying potential delays early.
4. Resources needed to complete the project
It’s crucial to recognize and list the resources you’ll need to complete the tasks. This can encompass financial resources, human resources, equipment, technological tool, marketing planning software or any other assets. Identifying these early ensures that there are no bottlenecks during execution due to a lack of necessary resources.
5. Person responsible
Assign a person or a team for each task. This designation ensures accountability and clarity. When individuals are aware of their responsibilities, it reduces overlap, confusion and ensures that every task has someone overseeing its completion.
6. Potential barriers or challenges
Every plan will face challenges. By anticipating potential barriers or obstacles, you can be better prepared to address them. This proactive approach ensures smoother execution and less reactionary problem-solving.
7. Measurement of key performance indicators (KPIs)
Determine how you’ll measure the success of each task or the plan overall. KPIs are tangible metrics that allow you to gauge progress and determine whether you’re moving closer to your goals and objectives. They offer a quantifiable means to evaluate success.
Action plans serve as blueprints, guiding the steps and resources needed to achieve a specific goal.
They come in various formats, tailored to different scenarios and objectives. Here, we present a range of action plan examples that cater to diverse purposes and situations.
From business strategies to simple task lists, these examples illustrate the versatility and importance of well-structured planning.
Business action plan example
A business action plan is essentially a strategy roadmap, meticulously tailored for realizing broader business objectives. By crafting a solid action plan, businesses can channel their resources, manpower and strategies in a direction that harmonizes with their larger vision.

Key to this plan is the identification and alignment of steps that resonate with the company’s comprehensive strategy, ambitions of growth and aspirations for operational enhancements.
While this might entail a myriad of specific steps based on unique business goals, some common elements include setting clear key performance indicators (KPIs), undertaking a thorough SWOT (Strengths, Weaknesses, Opportunities, Threats) analysis to grasp the current business landscape and establishing a timeline to keep track of progress.

Furthermore, allocating responsibilities to team members or individuals ensures that every aspect of the strategy has a dedicated focus. Budgeting, essential to the success of the action plan, ensures that every initiative is financially viable and sustainable.

Regular reviews and iterations based on feedback and changing market dynamics keep the action plan agile and relevant.
Related: 5 Steps to Create an Actionable Employee Development Plan [with Templates & Examples]
Company action plan example
A comprehensive company action plan serves as the strategic linchpin, ensuring a coherent and coordinated approach to realizing organizational goals. Central to this plan is the incorporation of rigorous market research and analysis, which provides insights into consumer behaviors, market trends and potential opportunities.

Equally vital is the focus on product development and procurement, ensuring that the offerings align with market demands and stand out in terms of quality and relevance.
Alongside, adept legal and financial management safeguards the company’s interests, ensuring compliance with regulations and prudent fiscal oversight.

Moreover, the essence of any successful company action plan lies in its sales and marketing strategies. These define how the products or services are positioned and promoted in the market, ensuring visibility and engagement with the target audience.

However, while acquisition is crucial, retention plays an equally significant role. Hence, impeccable customer service and nurturing relationships become indispensable components, fostering loyalty and ensuring that clients remain ambassadors for the brand long after the initial transaction.
Related: 30+ Project Plan Examples to Visualize Your Strategy (2023)
Sales action plan example
A well-structured sales action plan serves as the backbone for systematic and efficient progress. Central to this plan is the identification and utilization of the most effective sales channels, whether they are direct, online or through third-party avenues.

Clarity on the products and services on offer, combined with their unique selling propositions, facilitates tailored and resonant sales pitches.
Budget considerations ensure that resources are judiciously allocated, balancing the act between expenditures and potential returns. This financial prudence is complemented by setting realistic sales projections, which act as both a motivational target and a yardstick for success.
Timelines, or proposed deadlines, infuse the process with a sense of urgency, ensuring that the momentum of the sales drive is maintained.

However, the true measure of the action plan’s efficacy lies in its key performance indicators (KPIs). These metrics, be it lead conversion rates or customer retention figures, serve as tangible markers, highlighting the plan’s strengths and signaling areas that might require recalibration to increase sales.

Corrective action plan example
The essence of a corrective action plan lies in its meticulous structure, tailored to address and rectify deviations or inefficiencies identified within an organization. At its core, each action item serves as a focal point, detailing specific areas or processes that require intervention.

Accompanying each action item is a clear description that provides a comprehensive understanding of the issue at hand.
However, merely identifying a problem isn’t enough; delving deep into its origins through root cause analysis ensures that solutions target the fundamental issues, rather than just addressing superficial symptoms.

This analysis then paves the way for defining the corrective action, a tangible step or series of steps designed to mitigate the identified problem and prevent its recurrence.
Besides, to ensure the plan’s effectiveness, assigning a responsible person to each action item is paramount. This individual or team is entrusted with the task’s execution, ensuring accountability and focus.

The status of each action keeps stakeholders informed about the progress, be it in the planning phase, ongoing, or completed.
Lastly, setting a due date for each corrective action introduces a sense of urgency and purpose, ensuring that issues are addressed in a timely manner, minimizing disruptions and maximizing operational efficiency.
Simple action plan example
A simple action plan strips away the layers of complexity, offering a concise and direct approach to achieving a goal or addressing an issue. This type of plan is characterized by its straightforward structure, devoid of extraneous details, yet powerfully effective in its clarity.
It is specifically designed for tasks or objectives that don’t necessitate elaborate strategies or multi-layered approaches.

The core components of a simple action plan usually include a clear statement of the task or objective at hand, followed by a sequence of actions or steps to be taken.
Each step is described succinctly, ensuring that anyone involved has a clear understanding of what is expected. Responsibilities are defined clearly, with each task allocated to an individual or a team, ensuring accountability. Timelines might be integrated, providing a clear framework for completion, even if they’re just broad milestones.

Regular check-ins or assessments, although minimal, might be incorporated to monitor progress.
The beauty of a simple action plan lies in its agility and adaptability, making it particularly suited for individual projects, short-term tasks or situations where a rapid response is required.

How to write an action plan?
Creating an effective action plan is a foundational step towards turning aspirations into tangible results. It provides a clear roadmap, ensuring that each step taken aligns with the overall objective.
Whether you’re aiming to enhance a business process or achieve a personal goal, a well-drafted action plan can be your guiding light. Here’s key steps on how you can craft one:
- Step 1: Establish SMART goals: Initiating with a goal that is specific, measurable, achievable, relevant and time-bound ensures you have a clear and focused endpoint in sight. Smart goals serves as the cornerstone for your entire strategic blueprint.
- Step 2: Determine necessary tasks: Decompose your overarching objective into smaller, actionable tasks. This modular approach not only makes the mission less daunting but also provides a sequential pathway to goal attainment.
- Step 3: Assign essential resources: Depending on the tasks at hand, designate necessary resources, be they human, financial or technological. This ensures that every activity has the backing it needs for successful execution.
- Step 4: Prioritize tasks by importance: Not all tasks hold equal weight. Determine the hierarchy of tasks based on their impact on the goal and their time sensitivity. This allows for a systematic progression.
- Step 5: Outline timelines and key markers: With tasks in hand, set clear deadlines for each. Introduce milestones, which act as periodic check-ins, ensuring you’re on track and allowing for celebrations of smaller victories.
- Step 6: Oversee and modify your strategy blueprint: As you progress, there will invariably be learnings and challenges. Regularly review your plan to make necessary adjustments, ensuring its relevance and effectiveness.
- Step 7: Consider ready-to-use templates: If starting from scratch feels overwhelming, lean on structured templates to guide your planning. There’s plenty of business plan softwares and platforms such as Venngage that offer a plethora of action plan templates , tailored to various needs, which can significantly streamline the process.
An action plan is more than just an action steps, it’s a strategic blueprint that bridges the gap between aspirations and realizations.
Through this comprehensive guide, I’ve walked you through the purpose, ideal timings, core components, and practical examples of action plans across various domains.
Leveraging tools of project management , you can track progress, assign tasks and ensure every team member stays on the same page.
It’s not just about setting goals, but about strategically planning every step, ensuring tasks completed align with the larger project goals.
Remember, success isn’t just about having goals but about charting the right course to achieve them
And if you’re looking to supercharge your planning efforts, don’t miss out on the Venngage business plan maker.
Dive into their extensive collection of action plan templates and make your strategic planning both efficient and effective.
Discover popular designs

Infographic maker
Brochure maker
White paper online

Newsletter creator

Flyer maker
Timeline maker
Letterhead maker
Mind map maker

Ebook maker
- Contact sales
Start free trial
How to Write an Action Plan (Example Included)
What Is an Action Plan?
In project management, an action plan is a document that lists the action steps needed to achieve project goals and objectives. Therefore, an action plan clarifies what resources you’ll need to reach those goals, makes a timeline for the action items and determines what team members are required. We’ll define what project goals, project objectives, action items and action steps are later in this guide.
An action plan is similar to a project implementation plan, and it’s very helpful during the project planning and project execution phases. That’s because an action plan documents the execution of the project plan; it’s a detailed list of the work that must be done to complete the project goals, from the start of the project to the finish.
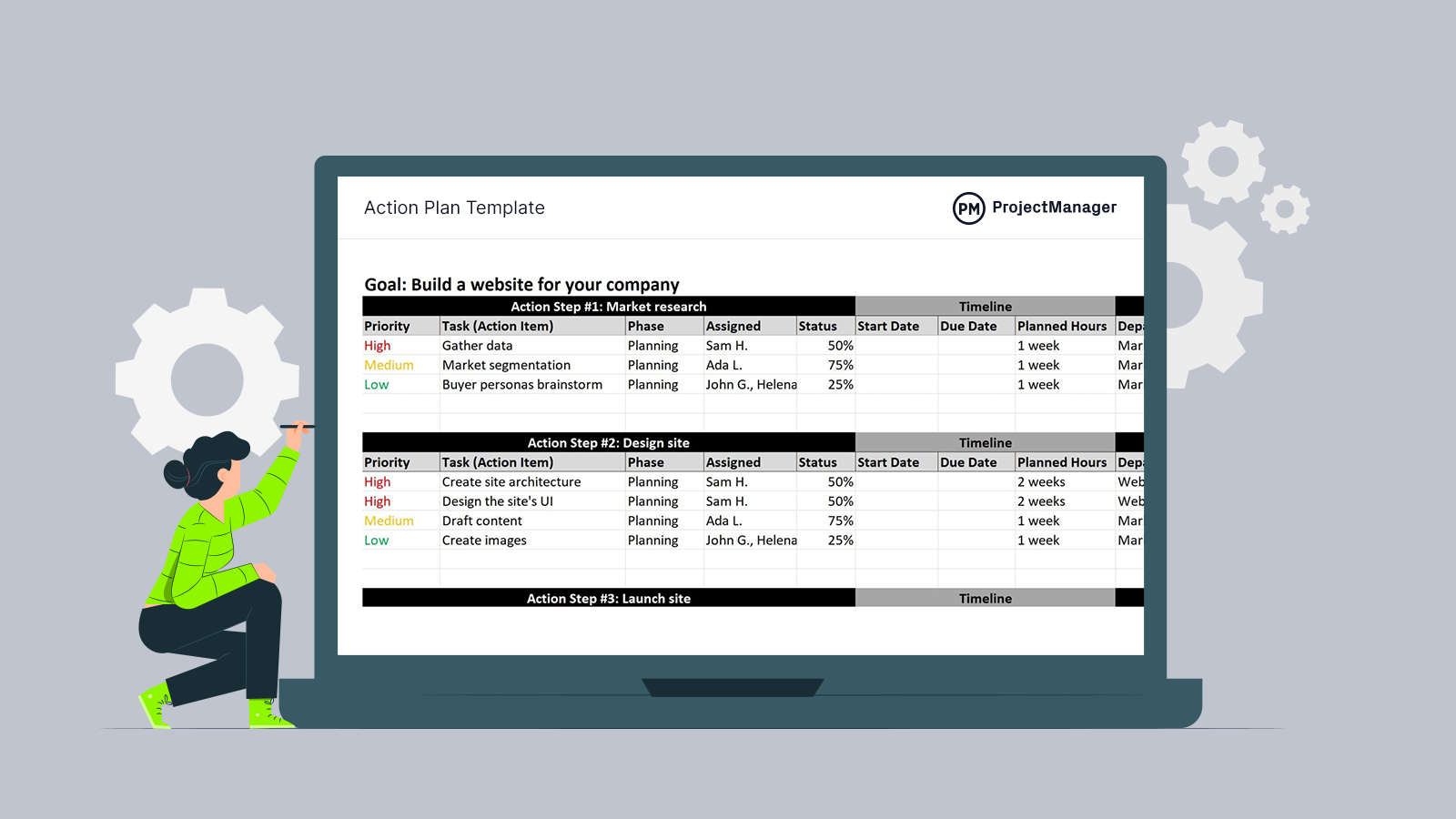
Action Plan Sample
Take a look at this sample of an action plan. We used our free action plan template for Excel and filled out some potential marketing tasks, phases and assignees. It’s a thorough action plan that accounts for progress, timelines, planned hours, resources and even costs. It’s a great place to start when making your own action plan. Download it and keep reading to make an ideal action plan.

Action Plan Components
An action plan answers the who, what and when of what you’re proposing. Those questions are answered by the various components that make up an action plan. The following are the basic building blocks of a successful action plan.
- Action Plan Steps: The action plan steps are the answer to the question of what. They’re the activities that’ll lead to achieving your goal. Action plan steps detail what will happen, and the more detail, the better.
- Action Items: The action items are the specific, small tasks that make up the action plan steps. These are the tasks that, when executed, lead to the next action plan step.
- Action Plan Timeline: An action plan timeline is the whole action plan laid out from start to finish. It shows the full duration of the action plan and every step and task is also plotted on this timeline, including their start and end dates.
- Action Plan Resources: Resources are anything needed to execute the action plan. That includes labor, materials, equipment, etc. You’ll want to identify the resources you’ll need for the action plan and attach them to the tasks to which they’ll be applied.
- Action Plan Matrix: A matrix is just a tool to help you determine which tasks you need to complete and in what order. Use our free action plan template to outline the steps, items, timeline and resources you’ll need to get the plan done right.
- Action Plan Report: Once you start to execute the action plan, you’ll need to ensure your actual progress matches your planned progress. To track progress, you’ll want to use an action plan report, which is a snapshot of your time, costs and more over a specific period.
Not only are you figuring out the action steps and timeline, but you’ll also determine who you’ll assemble for your project team to work on those tasks. This requires robust project management software like ProjectManager . ProjectManager offers multiple action planning tools such as Gantt charts, kanban boards, project calendars and more. Best of all, these project planning views sync with project dashboards, timesheets and workload charts to keep track of progress, project resources and costs.

Types of Action Plans
There are many different types of action plans that are used on various kinds of strategic initiatives. Each is similar in makeup but differs in their goals. Here are a few of the varieties of action plans.
Business Action Plan
A business action plan is used to set goals and tasks when you want to start a business or grow an existing business. It outlines the vision for the business and the actions you’ll take to achieve that vision.
Project Action Plan
An action plan for a project is really no different from a general action plan. The only difference is that it’s about producing a deliverable at the end of the plan, whether that be a product or service.
Personal Action Plan
Again, a personal action plan differs little from any other action plan except for the goal. For example, a personal action plan might be for an individual to exercise more. Therefore, the goal might be to walk for a half-hour a day, say, during lunchtime.
Get your free
Action Plan Template
Use this free Action Plan Template for Excel to manage your projects better.
How to Write an Action Plan for Project Management in 10 Steps
The benefits of an action plan are simple: you’ve now outlined what action steps and what resources are needed to reach your stated project goals. By having this collected in a single project management document, you can more successfully plan out how to execute your project plan.
People get overwhelmed by project management jargon when having to plan out a project, but the word “action” everyone can understand. The fundamentals to getting an action plan together for any project follow these four project planning basic steps:
1. Define Your Project Goals
There’s a difference between project goals and project objectives. Project goals refer to the high-level goals that the project will achieve. Those generally align with the strategic planning and business objectives of organizations.
2. Define Your Project Objectives
The project objectives are much more specific than the project goals. Project objectives refer to the deliverables and milestones that need to be completed to achieve your project goals.
3. Define Action Steps
The action steps are a group of related tasks or action items that must be executed to produce project deliverables.
4. Identify and Prioritize Action Items
Action items are small, individual tasks that make up the action steps that are outlined in your action plan. First, you need to identify task dependencies among them, and then assign those action items a priority level so that they’re executed sequentially.
5. Define Roles & Responsibilities
Now that you’ve divided the work required to accomplish your action plan, you’ll need to assign action items to your project team members and define their roles and responsibilities.

6. Allocate Resources
As with your project plan, your action plan has resource requirements. Having identified your action steps and action items will help you understand what resources are needed for each task and allocate them accordingly.
7. Set SMART Goals
Your action plan needs to be monitored and controlled to measure its performance. That’s why it’s important that you set SMART goals for your action items, action steps and your project objectives. SMART goals stand for specific, measurable, attainable, relevant and timely.
8. Set a Timeline for Your Action Plan
As a project manager, you’ll need to do your best to estimate how long it’ll take to complete your action items and action steps. Once you do so, you’ll have a timeline. You can use project management techniques like PERT charts or the critical path method to better estimate the duration of your project action plan.

9. Write an Action Plan Template
Create or use a simple action plan template to collect tasks, deadlines and assignments. This is the place where everything task-related goes in your project action plan, so you have a place for all this crucial information.
Writing an action plan template it’s a great idea because you’ll need to use that format throughout the project. That’s why we’ve created a free action plan template that you can download. There are also dozens of other free project management templates for Excel and Word that can help you with every phase of your project.
10. Use a Project Management Tool
Use a project management tool to keep you on task. ProjectManager has project planning features that help you monitor and report on project progress and performance. Get a high-level view of the action plan with our live dashboards. Unlike other tools, we don’t make you set up the dashboard.
Once you’ve mapped out your action plan, you can use project planning tools to zoom into all the details about your action steps and action items. With ProjectManager, you can calculate various metrics, such as project variance, workload and more. They’re displayed in easy-to-read charts and graphs. Share them with stakeholders to give them updates on action steps whenever they want.

Tips to Write an Action Plan
Once you have an action plan, how do you work with it to run a successful project? Here are some tips to help with implementing your action plan:
- Focus on priorities and what’s due now when identifying action steps and setting your action plan timeline
- When you complete action steps, mark them off
- Have your team members work on one project management platform
- Set up alerts
- Discuss pending or overdue tasks
Action Plan Example
We’ve been talking a lot about an action plan, but let’s take a look at one in-depth. Below, you’ll see our free action plan template . It’s set up for the development of a website.
It’s broken down into phases, the first being the project planning phase , which includes the action steps, market research and the design of the site. You’ll see that tasks are outlined for each action step, including a description of that task, who’s assigned to execute it, the priority and even the status of its completion.
This is followed by the third action step, which is the launch of the site. This is the execution phase of the action plan, but it follows the same format, such as noting the priority, who’s responsible for the work, what that work is and its status.

There’s also a timeline to define the start dates of each of the tasks in the action steps, including the planned hours. This allows you to determine the length of each task and the duration of the entire action plan, from start to finish.

Finally, there’s a place to add your resources. They’re broken down into departments, for example, marketing, web development, etc. Then the materials that are required for each task are listed, including their costs. This allows you to estimate the cost of the plan.

How to Make An Action Plan With ProjectManager
Follow along with this action plan example to see how action plans are typically laid out using project planning software .
1. Map Action Plan Steps Using Multiple Project Views
ProjectManager can help you build your action plan and then execute it. Collect all your action steps tasks on our list view, which does more than light-weight to-do list apps because it allows you to then map your action plan with Gantt charts , project calendars and kanban boards. These robust project management tools allow you to prioritize action items, customize tags and show the percentage complete for each task. Our online project management software gives you real-time data to help you create an action plan and stick to it.

2. Assign Action Items to Your Team Members
Once you’ve mapped out your action plan steps with ProjectManager’s project planning tools , you can assign tasks to your team members and indicate what resources are needed for the completion of each action item. Indicate their roles and responsibilities and set priority levels for each task to ensure the work is carried out properly.
3. Set Action Plan Steps and Deliverables
It’s important to note all the phases of the project timeline to know what action steps and tasks will take place and when. In addition, ProjectManager’s Gantt chart allows you to identify project phases, find the critical path, and set due dates for project milestones and deliverables
4. Track Progress With Real-Time Dashboards
Once you start the project, you’ll need to chart the progress of the work being done. This leads us to the real-time project dashboard , where you’ll check whether your action plan is on schedule and under budget.
Manage Your Project With an Action Plan
Getting a plan together is only the first part of managing a project . Remember, it’s not something to write and put away, but rather it’s a living document that should follow you throughout the project life cycle. Jennifer Bridges, PMP, offers more tips on how to write an action plan in the video below.
Here’s a screenshot for your reference:

ProjectManager’s Action Planning Tools are Ideal for Managing Action Plans
If you’re looking to make an action plan and then take action on it by executing, monitoring and reporting on a project, then you’ll want ProjectManager. Our online project management software lets you make an action plan online with multiple project planning tools such as Gantt charts, task lists, kanban boards and project calendars. Then, you can use timesheets, project dashboards and resource management tools to keep track of progress, time and costs.
Plan & Schedule With Gantt Charts
ProjectManager’s Gantt chart is ideal to map out your action plan on an interactive project timeline that helps you organize your tasks, link dependencies and set milestones. More than that, you can filter for the critical path. When you’re done scheduling your action steps you can set a baseline. This allows you to always see the planned versus actual progress of your action plan to help you stay on track.

Manage Action Items with Kanban Boards, Task Lists and Project Calendars
Once you’ve used the Gantt chart to create a timeline for your action plan, you can zoom into the nitty-gritty details of everyday work with kanban boards , task lists and project calendars. With these tools, you can assign tasks and give teams a collaborative platform to comment and share relevant documents with unlimited file storage and real-time communication features.

Track Progress, Resources and Costs With Real-Time Action Plan Dashboards
ProjectManager’s real-time action plan dashboards sync with all its project management tools so you can check the status of your action plan at any time. You can check on your team members’ progress to see who’s over or underallocated, check labor costs and track whether your team is on schedule.

ProjectManager gives you all the tools you need to create and implement a successful action plan. Regardless of the type of action plan that you need to create, our award-winning project management software makes it easy to do so. Get started with a free 30-day trial today.

Deliver your projects on time and on budget
Start planning your projects.
What is an Action Plan? Learn with Templates and Examples
Planning on turning your vision into reality? And what’s your best way to avoid challenges and problems during this journey? A solid action plan.
We have outlined 6 steps explaining how to write an action plan. Once you familiarize yourself with them, go ahead and use the editable templates below to start planning right away.
What is an Action Plan?
Why you need an action plan, how to write an action plan, action plan templates.
An action plan is a specific list of tasks in order to achieve a particular goal. It can be regarded as a proposed strategy to execute a specific project to achieve a specific or general goal effectively and efficiently. It outlines steps to take and helps stay focused and organized, whether it’s personal or work-related. Breaking down the goal into smaller, manageable steps, makes it easier to stay motivated and track progress.
It’s an essential part of the strategic planning process and helps with improving teamwork planning Not only in project management, but action plans can be used by individuals to prepare a strategy to achieve their own personal goals as well.
Components of an action plan include
- A well-defined description of the goal to be achieved
- Tasks/ steps that need to be carried out to reach the goal
- People who will be in charge of carrying out each task
- When will these tasks be completed (deadlines and milestones)
- Resources needed to complete the tasks
- Measures to evaluate progress
What’s great about having everything listed down on one location is that it makes it easier to track progress and effectively plan things out.
An action plan is not something set in stone. As your organization grows, and surrounding circumstances change, you will have to revisit and make adjustments to meet the latest needs.
Sometimes businesses don’t spend much time on developing an action plan before an initiative, which, in most cases, leads to failure. If you haven’t heard, “failing to plan is planning to fail” said Benjamin Franklin supposedly once.
Planning helps you prepare for the obstacles ahead and keep you on track. And with an effective action plan, you can boost your productivity and keep yourself focused.
Here are some benefits of an action plan you should know;
- It gives you a clear direction. As an action plan highlights exactly what steps to be taken and when they should be completed, you will know exactly what you need to do.
- Having your goals written down and planned out in steps will give you a reason to stay motivated and committed throughout the project.
- With an action plan, you can track your progress toward your goal.
- Since you are listing down all the steps you need to complete in your action plan, it will help you prioritize your tasks based on effort and impact.
From the looks of it, creating an action plan seems fairly easy. But there are several important steps you need to follow with caution in order to get the best out of it. Here’s how to write an action plan explained in 6 easy steps.
Step 1: Define your end goal
If you are not clear about what you want to do and what you want to achieve, you are setting yourself up for failure.
Planning a new initiative? Start by defining where you are and where you want to be.
Solving a problem? Analyze the situation and explore possible solutions before prioritizing them.
Then write down your goal. And before you move on to the next step, run your goal through the SMART criteria . Or in other words, make sure that it is
- Specific – well-defined and clear
- Measurable – include measurable indicators to track progress
- Attainable – realistic and achievable within the resources, time, money, experience, etc. you have
- Relevant – align with your other goals
- Timely – has a finishing date
Use this SMART goal worksheet to simplify this process. Share it with others to get their input as well.
- Ready to use
- Fully customizable template
- Get Started in seconds

And refer to our easy guide to the goal-setting process to learn more about setting and planning your goals.
Step 2: List down the steps to be followed
The goal is clear. What exactly should you do to realize it?
Create a rough template to list down all the tasks to be performed, due dates and people responsible.
It’s important that you make sure that the entire team is involved in this process and has access to the document. This way everyone will be aware of their roles and responsibilities in the project.
Make sure that each task is clearly defined and is attainable. If you come across larger and more complex tasks, break them down to smaller ones that are easier to execute and manage.
Tips: Use a RACI Matrix template to clarify project roles and responsibilities, and plan projects
Step 3: Prioritize tasks and add deadlines
It’s time to reorganize the list by prioritizing the tasks . Some steps, you may need to prioritize as they can be blocking other sub-steps.
Add deadlines, and make sure that they are realistic. Consult with the person responsible for carrying it out to understand his or her capacity before deciding on deadlines.
Step 4: Set milestones
Milestones can be considered mini goals leading up to the main goal at the end. The advantage of adding milestones is that they give the team members to look forward to something and help them stay motivated even though the final due date is far away.
Start from the end goal and work your way back as you set milestones . Remember not to keep too little or too much time in between the milestone you set. It’s a best practice to space milestones two weeks apart.
Step 5: Identify the resources needed
Before you start your project, it’s crucial to ensure that you have all the necessary resources at hand to complete the tasks. And if they are not currently available, you need to first make a plan to acquire them.
This should also include your budget. You can assign a column of your action plan to mark the cost of each task if there are any.
Step 6: Visualize your action plan
The point of this step is to create something that everyone can understand at a glance and that can be shared with everyone.
Whether your action plan comes in the shape of a flowchart , Gantt chart , or table , make sure that it clearly communicates the elements we have identified so far – tasks, task owners, deadlines, resources, etc.
This document should be easily accessible to everyone and should be editable.
Step 7: Monitor, evaluate and update
Allocate some time to evaluate the progress you’ve made with your team.
You can mark tasks that are completed as done on this final action plan, bringing attention to how you’ve progressed toward the goal.
This will also bring out the tasks that are pending or delayed, in which case you need to figure out why and find suitable solutions. And then update the action plan accordingly.
Business action plan
You may like to read: The Easy Guide to Making a Business Plan for Presentations
Marketing action plan
Strategic action plan, corrective action plan template.
Learn more about: Corrective Action Plan template .
Additional resources: The Easy Guide to Creating a Business Contingency Plan
Simple action plan template
Any more tips on creating an action plan.
An action plan is designed to guide your way to accomplishing your goals. It turns your vision into actionable goals and steps. And it helps you stay focused and motivated.
From an individual employee in an organization to larger departments can make use of action plans to steer their way towards completing their goals.
Maybe you are about to create your very first action plan, or you are already a pro at writing them. Either way, we’d like to hear your opinions on how to write an action plan. Do share them with us in the comments section below.
Join over thousands of organizations that use Creately to brainstorm, plan, analyze, and execute their projects successfully.
FAQs About Action Plan
Lack of clarity on goals: Make sure the team understands the goals and objectives of the action plan. The goals should be specific, measurable, attainable, relevant, and time-bound (SMART).
Unclear responsibilities: Assign clear roles and responsibilities for each team member to avoid confusion and ensure accountability.
Overcomplicating the plan: Keep the action plan simple and easy to understand. Avoid adding unnecessary complexity or detail that may confuse the team.
Failure to prioritize tasks: Prioritize tasks based on their importance and urgency. This will ensure that the team focuses on the most critical tasks first.
Inadequate resources: Ensure that the team has access to the necessary resources such as time, budget, and equipment, to carry out the action plan successfully.
Lack of communication: Effective communication is crucial to the success of any action plan. Ensure that team members are regularly updated on progress and any changes to the plan.
Failure to monitor progress: Regularly monitor progress and adjust the action plan as needed to ensure that it stays on track and achieves its goals.
Strategic action plan: This type of plan outlines the long-term goals and objectives of an organization, and the actions that will be taken to achieve them. It typically covers a period of several years and includes high-level strategies and initiatives.
Operational action plan: This plan focuses on the day-to-day operations of an organization, outlining the actions that will be taken to achieve short-term goals and objectives. It typically covers a period of one year or less and includes specific actions and timelines.
Project action plan: This type of plan is used for individual projects and outlines the actions that will be taken to achieve specific project goals and objectives. It includes a detailed breakdown of tasks, timelines, and responsibilities.
Sales action plan: This plan focuses on the actions that will be taken to increase sales and revenue. It includes specific strategies for marketing, sales, and customer service.
Marketing action plan: This plan outlines the actions that will be taken to promote a product or service and increase brand awareness. It includes strategies for advertising, social media, public relations, and other marketing initiatives.
Crisis management action plan: This type of plan outlines the actions that will be taken in the event of a crisis, such as a natural disaster or security breach. It includes specific protocols for communication, evacuation, and other emergency procedures.
An action plan can be used by anyone who wants to achieve specific goals or objectives. It is a useful tool for individuals, teams, and organizations in a variety of contexts. Here are some examples:
Individuals: An individual can use an action plan to achieve personal goals such as losing weight, completing a degree, or starting a business.
Teams: A team can use an action plan to achieve goals related to a specific project or initiative. For example, a marketing team may use an action plan to launch a new product.
Small businesses: Small businesses can use an action plan to achieve goals related to sales, marketing, operations, or finance.
Non-profit organizations: Non-profit organizations can use an action plan to achieve goals related to fundraising, volunteer recruitment, or program implementation.
Government agencies: Government agencies can use an action plan to achieve goals related to policy implementation, disaster response, or public safety.
Educational institutions: Educational institutions can use an action plan to achieve goals related to improving student outcomes, increasing enrollment, or expanding programs.
More Related Articles

Amanda Athuraliya is the communication specialist/content writer at Creately, online diagramming and collaboration tool. She is an avid reader, a budding writer and a passionate researcher who loves to write about all kinds of topics.
How to Write a Case Study: A Step-by-Step Guide (+ Examples)
by Todd Brehe
on Jan 3, 2024
If you want to learn how to write a case study that engages prospective clients, demonstrates that you can solve real business problems, and showcases the results you deliver, this guide will help.
We’ll give you a proven template to follow, show you how to conduct an engaging interview, and give you several examples and tips for best practices.
Let’s start with the basics.
What is a Case Study?
A business case study is simply a story about how you successfully delivered a solution to your client.
Case studies start with background information about the customer, describe problems they were facing, present the solutions you developed, and explain how those solutions positively impacted the customer’s business.
Do Marketing Case Studies Really Work?
Absolutely. A well-written case study puts prospective clients into the shoes of your paying clients, encouraging them to engage with you. Plus, they:
- Get shared “behind the lines” with decision makers you may not know;
- Leverage the power of “social proof” to encourage a prospective client to take a chance with your company;
- Build trust and foster likeability;
- Lessen the perceived risk of doing business with you and offer proof that your business can deliver results;
- Help prospects become aware of unrecognized problems;
- Show prospects experiencing similar problems that possible solutions are available (and you can provide said solutions);
- Make it easier for your target audience to find you when using Google and other search engines.
Case studies serve your clients too. For example, they can generate positive publicity and highlight the accomplishments of line staff to the management team. Your company might even throw in a new product/service discount, or a gift as an added bonus.
But don’t just take my word for it. Let’s look at a few statistics and success stories:
5 Winning Case Study Examples to Model
Before we get into the nuts and bolts of how to write a case study, let’s go over a few examples of what an excellent one looks like.
The five case studies listed below are well-written, well-designed, and incorporate a time-tested structure.
1. Lane Terralever and Pinnacle at Promontory

This case study example from Lane Terralever incorporates images to support the content and effectively uses subheadings to make the piece scannable.
2. WalkMe Mobile and Hulyo

This case study from WalkMe Mobile leads with an engaging headline and the three most important results the client was able to generate.
In the first paragraph, the writer expands the list of accomplishments encouraging readers to learn more.
3. CurationSuite Listening Engine

This is an example of a well-designed printable case study . The client, specific problem, and solution are called out in the left column and summarized succinctly.
4. Brain Traffic and ASAE

This long format case study (6 pages) from Brain Traffic summarizes the challenges, solutions, and results prominently in the left column. It uses testimonials and headshots of the case study participants very effectively.
5. Adobe and Home Depot

This case study from Adobe and Home Depot is a great example of combining video, attention-getting graphics, and long form writing. It also uses testimonials and headshots well.
Now that we’ve gone over the basics and showed a few great case study examples you can use as inspiration, let’s roll up our sleeves and get to work.
A Case Study Structure That Pros Use
Let’s break down the structure of a compelling case study:
Choose Your Case Study Format
In this guide, we focus on written case studies. They’re affordable to create, and they have a proven track record. However, written case studies are just one of four case study formats to consider:
- Infographic
If you have the resources, video (like the Adobe and Home Depot example above) and podcast case studies can be very compelling. Hearing a client discuss in his or her own words how your company helped is an effective content marketing strategy
Infographic case studies are usually one-page images that summarize the challenge, proposed solution, and results. They tend to work well on social media.
Follow a Tried-and-True Case Study Template
The success story structure we’re using incorporates a “narrative” or “story arc” designed to suck readers in and captivate their interest.
Note: I recommend creating a blog post or landing page on your website that includes the text from your case study, along with a downloadable PDF. Doing so helps people find your content when they perform Google and other web searches.
There are a few simple SEO strategies that you can apply to your blog post that will optimize your chances of being found. I’ll include those tips below.
Craft a Compelling Headline
The headline should capture your audience’s attention quickly. Include the most important result you achieved, the client’s name, and your company’s name. Create several examples, mull them over a bit, then pick the best one. And, yes, this means writing the headline is done at the very end.
SEO Tip: Let’s say your firm provided “video editing services” and you want to target this primary keyword. Include it, your company name, and your client’s name in the case study title.
Write the Executive Summary
This is a mini-narrative using an abbreviated version of the Challenge + Solution + Results model (3-4 short paragraphs). Write this after you complete the case study.
SEO Tip: Include your primary keyword in the first paragraph of the Executive Summary.
Provide the Client’s Background
Introduce your client to the reader and create context for the story.
List the Customer’s Challenges and Problems
Vividly describe the situation and problems the customer was dealing with, before working with you.
SEO Tip: To rank on page one of Google for our target keyword, review the questions listed in the “People also ask” section at the top of Google’s search results. If you can include some of these questions and their answers into your case study, do so. Just make sure they fit with the flow of your narrative.
Detail Your Solutions
Explain the product or service your company provided, and spell out how it alleviated the client’s problems. Recap how the solution was delivered and implemented. Describe any training needed and the customer’s work effort.
Show Your Results
Detail what you accomplished for the customer and the impact your product/service made. Objective, measurable results that resonate with your target audience are best.
List Future Plans
Share how your client might work with your company in the future.
Give a Call-to-Action
Clearly detail what you want the reader to do at the end of your case study.
Talk About You
Include a “press release-like” description of your client’s organization, with a link to their website. For your printable document, add an “About” section with your contact information.
And that’s it. That’s the basic structure of any good case study.
Now, let’s go over how to get the information you’ll use in your case study.
How to Conduct an Engaging Case Study Interview
One of the best parts of creating a case study is talking with your client about the experience. This is a fun and productive way to learn what your company did well, and what it can improve on, directly from your customer’s perspective.
Here are some suggestions for conducting great case study interviews:
When Choosing a Case Study Subject, Pick a Raving Fan
Your sales and marketing team should know which clients are vocal advocates willing to talk about their experiences. Your customer service and technical support teams should be able to contribute suggestions.
Clients who are experts with your product/service make solid case study candidates. If you sponsor an online community, look for product champions who post consistently and help others.
When selecting a candidate, think about customer stories that would appeal to your target audience. For example, let’s say your sales team is consistently bumping into prospects who are excited about your solution, but are slow to pull the trigger and do business with you.
In this instance, finding a client who felt the same way, but overcame their reluctance and contracted with you anyway, would be a compelling story to capture and share.
Prepping for the Interview
If you’ve ever seen an Oprah interview, you’ve seen a master who can get almost anyone to open up and talk. Part of the reason is that she and her team are disciplined about planning.
Before conducting a case study interview, talk to your own team about the following:
- What’s unique about the client (location, size, industry, etc.) that will resonate with our prospects?
- Why did the customer select us?
- How did we help the client?
- What’s unique about this customer’s experience?
- What problems did we solve?
- Were any measurable, objective results generated?
- What do we want readers to do after reading this case study analysis?
Pro Tip: Tee up your client. Send them the questions in advance.
Providing questions to clients before the interview helps them prepare, gather input from other colleagues if needed, and feel more comfortable because they know what to expect.
In a moment, I’ll give you an exhaustive list of interview questions. But don’t send them all. Instead, pare the list down to one or two questions in each section and personalize them for your customer.
Nailing the Client Interview
Decide how you’ll conduct the interview. Will you call the client, use Skype or Facetime, or meet in person? Whatever mode you choose, plan the process in advance.
Make sure you record the conversation. It’s tough to lead an interview, listen to your contact’s responses, keep the conversation flowing, write notes, and capture all that the person is saying.
A recording will make it easier to write the client’s story later. It’s also useful for other departments in your company (management, sales, development, etc.) to hear real customer feedback.
Use open-ended questions that spur your contact to talk and share. Here are some real-life examples:
Introduction
- Recap the purpose of the call. Confirm how much time your contact has to talk (30-45 minutes is preferable).
- Confirm the company’s location, number of employees, years in business, industry, etc.
- What’s the contact’s background, title, time with the company, primary responsibilities, and so on?
Initial Challenges
- Describe the situation at your company before engaging with us?
- What were the initial problems you wanted to solve?
- What was the impact of those problems?
- When did you realize you had to take some action?
- What solutions did you try?
- What solutions did you implement?
- What process did you go through to make a purchase?
- How did the implementation go?
- How would you describe the work effort required of your team?
- If training was involved, how did that go?
Results, Improvements, Progress
- When did you start seeing improvements?
- What were the most valuable results?
- What did your team like best about working with us?
- Would you recommend our solution/company? Why?
Future Plans
- How do you see our companies working together in the future?
Honest Feedback
- Our company is very focused on continual improvement. What could we have done differently to make this an even better experience?
- What would you like us to add or change in our product/service?
During the interview, use your contact’s responses to guide the conversation.
Once the interview is complete, it’s time to write your case study.
How to Write a Case Study… Effortlessly
Case study writing is not nearly as difficult as many people make it out to be. And you don’t have to be Stephen King to do professional work. Here are a few tips:
- Use the case study structure that we outlined earlier, but write these sections first: company background, challenges, solutions, and results.
- Write the headline, executive summary, future plans, and call-to-action (CTA) last.
- In each section, include as much content from your interview as you can. Don’t worry about editing at this point
- Tell the story by discussing their trials and tribulations.
- Stay focused on the client and the results they achieved.
- Make their organization and employees shine.
- When including information about your company, frame your efforts in a supporting role.
Also, make sure to do the following:
Add Testimonials, Quotes, and Visuals
The more you can use your contact’s words to describe the engagement, the better. Weave direct quotes throughout your narrative.
Strive to be conversational when you’re writing case studies, as if you’re talking to a peer.
Include images in your case study that visually represent the content and break up the text. Photos of the company, your contact, and other employees are ideal.
If you need to incorporate stock photos, here are three resources:
- Deposit p hotos
And if you need more, check out Smart Blogger’s excellent resource: 17 Sites with High-Quality, Royalty-Free Stock Photos .
Proofread and Tighten Your Writing
Make sure there are no grammar, spelling, or punctuation errors. If you need help, consider using a grammar checker tool like Grammarly .
My high school English teacher’s mantra was “tighten your writing.” She taught that impactful writing is concise and free of weak, unnecessary words . This takes effort and discipline, but will make your writing stronger.
Also, keep in mind that we live in an attention-diverted society. Before your audience will dive in and read each paragraph, they’ll first scan your work. Use subheadings to summarize information, convey meaning quickly, and pull the reader in.
Be Sure to Use Best Practices
Consider applying the following best practices to your case study:
- Stay laser-focused on your client and the results they were able to achieve.
- Even if your audience is technical, minimize the use of industry jargon . If you use acronyms, explain them.
- Leave out the selling and advertising.
- Don’t write like a Shakespearean wannabe. Write how people speak. Write to be understood.
- Clear and concise writing is not only more understandable, it inspires trust. Don’t ramble.
- Weave your paragraphs together so that each sentence is dependent on the one before and after it.
- Include a specific case study call-to-action (CTA).
- A recommended case study length is 2-4 pages.
- Commit to building a library of case studies.
Get Client Approval
After you have a final draft, send it to the client for review and approval. Incorporate any edits they suggest.
Use or modify the following “Consent to Publish” form to get the client’s written sign-off:
Consent to Publish
Case Study Title:
I hereby confirm that I have reviewed the case study listed above and on behalf of the [Company Name], I provide full permission for the work to be published, in whole or in part, for the life of the work, in all languages and all formats by [Company publishing the case study].
By signing this form, I affirm that I am authorized to grant full permission.
Company Name:
E-mail Address:
Common Case Study Questions (& Answers)
We’ll wrap things up with a quick Q&A. If you have a question I didn’t answer, be sure to leave it in a blog comment below.
Should I worry about print versions of my case studies?
Absolutely.
As we saw in the CurationSuite and Brain Traffic examples earlier, case studies get downloaded, printed, and shared. Prospects can and will judge your book by its cover.
So, make sure your printed case study is eye-catching and professionally designed. Hire a designer if necessary.
Why are good case studies so effective?
Case studies work because people trust them.
They’re not ads, they’re not press releases, and they’re not about how stellar your company is.
Plus, everyone likes spellbinding stories with a hero [your client], a conflict [challenges], and a riveting resolution [best solution and results].
How do I promote my case study?
After you’ve written your case study and received the client’s approval to use it, you’ll want to get it in front of as many eyes as possible.
Try the following:
- Make sure your case studies can be easily found on your company’s homepage.
- Tweet and share the case study on your various social media accounts.
- Have your sales team use the case study as a reason to call on potential customers. For example: “Hi [prospect], we just published a case study on Company A. They were facing some of the same challenges I believe your firm is dealing with. I’m going to e-mail you a copy. Let me know what you think.”
- Distribute printed copies at trade shows, seminars, or during sales presentations.
- If you’re bidding on a job and have to submit a quote or a Request for Proposal (RFP), include relevant case studies as supporting documents.
Ready to Write a Case Study That Converts?
If you want to stand out and you want to win business, case studies should be an integral part of your sales and marketing efforts.
Hopefully, this guide answered some of your questions and laid out a path that will make it faster and easier for your team to create professional, sales-generating content.
Now it’s time to take action and get started. Gather your staff, select a client, and ask a contact to participate. Plan your interview and lead an engaging conversation. Write up your client’s story, make them shine, and then share it.
Get better at the case study process by doing it more frequently. Challenge yourself to write at least one case study every two months.
As you do, you’ll be building a valuable repository of meaningful, powerful content. These success stories will serve your business in countless ways, and for years to come.

Todd A. Brehe is a professional B2B freelance writer helping SaaS companies create sales-generating case studies, white papers, and blog content. Check out his work or contact him at: https://toddbrehe.com .
Content Marketing

The ultimate toolkit for becoming one of the highest-paid writers online. Premium training. Yours for free.

Written by Todd Brehe
6 thoughts on “how to write a case study: a step-by-step guide (+ examples)”.
Just the guide I needed for case studies! Great job with this one!
Hey Todd, great post here. I liked that you listed some prompting questions. Really demonstrates you know what you’re talking about. There are a bunch of Ultimate Guides out there who list the theories such as interview your customer, talk about results, etc. but really don’t help you much.
Thanks, Todd. I’ve planned a case study and this will really come in handy. Bookmarked.
Very good read. Thanks, Todd. Are there any differences between a case study and a use case, by the way?
Hi Todd, Very well-written article. This is the ultimate guide I have read till date. It has actionable points rather than some high-level gyan. Creating a new case study always works better when (1) you know the structure to follow and (2) you work in a group of 3-4 members rather than individually. Thanks for sharing this guide.
Hi Todd. Very useful guide. I learn step by step. Looking forward to continually learning from you and your team. Thanks
Leave a Comment Cancel reply
Latest from the blog.

How to Write a Book in 2024: Everything You Need to Know

How to Create a Swipe File: A Guide for Bloggers & Writers

What is Freelance Copywriting? & How to Get Started in 2024
With over 300k subscribers and 4 million readers, Smart Blogger is one of the world's largest websites dedicated to writing and blogging.
Best of the Blog
© 2012-2024 Smart Blogger — Boost Blog Traffic, Inc.
Terms | Privacy Policy | Refund Policy | Affiliate Disclosure
- Product overview
- All features
- Latest feature release
- App integrations
CAPABILITIES
- project icon Project management
- Project views
- Custom fields
- Status updates
- goal icon Goals and reporting
- Reporting dashboards
- workflow icon Workflows and automation
- portfolio icon Resource management
- Capacity planning
- Time tracking
- my-task icon Admin and security
- Admin console
- asana-intelligence icon Asana AI
- list icon Personal
- premium icon Starter
- briefcase icon Advanced
- Goal management
- Organizational planning
- Campaign management
- Creative production
- Content calendars
- Marketing strategic planning
- Resource planning
- Project intake
- Product launches
- Employee onboarding
- View all uses arrow-right icon
- Project plans
- Team goals & objectives
- Team continuity
- Meeting agenda
- View all templates arrow-right icon
- Work management resources Discover best practices, watch webinars, get insights
- Customer stories See how the world's best organizations drive work innovation with Asana
- Help Center Get lots of tips, tricks, and advice to get the most from Asana
- Asana Academy Sign up for interactive courses and webinars to learn Asana
- Developers Learn more about building apps on the Asana platform
- Community programs Connect with and learn from Asana customers around the world
- Events Find out about upcoming events near you
- Partners Learn more about our partner programs
- Asana for nonprofits Get more information on our nonprofit discount program, and apply.
Featured Reads

- Create an action plan that drives resul ...
Create an action plan that drives results

An action plan outlines precisely how you’re planning to accomplish your goals. It’s the perfect way to approach goals systematically and keep your team on target. In this article, we will cover how to create an action plan in six steps and how to implement it successfully. Plus, learn more about the differences between action plans, project plans, and to-do lists.
It can feel good to make goals. After all, you’re defining what you want to accomplish. But goals won’t do much without clear action steps. An action plan is a popular project management technique that lists your action steps so you know exactly how you’re going to accomplish your goals.
We’re going to show you how to create this clear roadmap step by step and other tools you should utilize to get the most out of your action plan. Let’s dive in.
What is an action plan?
An action plan is a list of tasks or steps you need to complete to achieve your goals. An effective action plan works like a management plan for your company’s initiatives, outlining the steps you need to take to make these larger goals a success. Once you go through the goal-setting process, create an action plan with specific tasks and timeframes to reach each goal.
Discover the future of workflow automation
Leverage AI-driven solutions to unleash your team's potential with dynamic workflows that adapt to ever-changing business needs and drive company-wide success.
Who needs an action plan?
An action plan is useful for anyone who needs a step-by-step planning process. When you create an action plan, you detail exactly what actions you'll take to accomplish your project goals. These plans can help you organize your to-dos and ensure you have the necessary information and resources to accomplish your goals.
But you can create action plans for more than just strategic planning. Use this tool to reach any specific goals in a systematic way. Try setting up:
Business action plan
Marketing action plan
Corrective action plan
Sales action plan
Project action plan
Personal development action plan
Regardless of the type of action plan you create, make sure you create it in task management software . That way, you can easily share action items and timelines with your team to track progress. Instead of manual status updates and unclear deliverables, your team has one central source of truth for everything they need to do in order to hit their goals.
Now let’s get into how you can create an action plan that increases your team’s efficiency and accountability.

6 steps to create an action plan
Step 1: set a smart goal.
When it comes to setting goals, clarity is the single most important quality. With the SMART goal method, your goal is clearly defined and attainable. Set specific, measurable, achievable, realistic, and time-bound goals to benefit from this tactic.
![[Inline illustration] SMART goals (Infographic)](https://assets.asana.biz/transform/bca4c26d-0f4a-4850-b9a3-ff698d140b19/inline-project-management-project-management-phases-2-2x?io=transform:fill,width:2560&format=webp "action plan for case study")
For example, your goal could be to deliver your current project (measurable) in four months (time-bound) without overspending (specific). Assuming this goal is both achievable and realistic based on your available resources, it’s a great SMART goal to set for yourself.
Step 2: Identify tasks
Now that your goal is clearly defined and written down, you’ll want to identify the steps you have to take to reach it. Identify all of the tasks that you and your team need to complete to reach milestones and, eventually, the main objective.
Here are a few action plan examples with tasks for different kinds of goals:
Goal: Expand team from seven to nine team members by June.
Meet with Human Resources to discuss the recruitment campaign.
Create a template project to track candidates.
Schedule three interviews per week.
Goal: Select and onboard new work management software to the entire company by the end of Q2.
Apply for the budget.
Create a roll-out plan for Q2.
Schedule training for team members.
Goal: Host 5k charity run in May to raise $15,000 for the local food bank.
Find volunteers and determine responsibilities
Prepare marketing materials and PR plans
Secure sponsors
Step 3: Allocate resources
Once you’ve outlined all of your tasks, you can allocate resources like team members, project budget, or necessary equipment. Whether it’s assigning team members to certain tasks, applying for a budget, or gathering helpful tools—now is the time to plan and prepare.
Sometimes, you can’t allocate all of your resources before you put your action plan in motion. Perhaps you have to apply for funding first or need executive approval before you can move on with a task. In that case, make the resource an action item in your plan so you can take care of it later.
Step 4: Prioritize tasks
When your team is clear on their priorities, they know what work to do first and what work they can reschedule if necessary. No action plan is set in stone, so the best way to empower your team is to let them know what tasks have a high priority and which ones are a bit more flexible.
To make this clear, sort all of your action items by priority and sequence:
Priority: Important and less important tasks.
Sequence: Order in which tasks have to be completed so others can start.
When you’re organizing and prioritizing your action items , you’ll notice that some action items are dependent on others. In other words, one task can’t begin until the previous task is completed. Highlight these dependencies and factor the sequence into your prioritization. This reduces bottlenecks , removing obstacles that would make a less important action item delay a high-priority item.
Step 5: Set deadlines and milestones
When your team knows what they're working towards, they have the context to effectively prioritize work and the motivation to get great work done. Team members tend to be more motivated when they directly understand how their work is contributing to larger goals.
To engage your teammates from the get go, assign deadlines to all action items and define milestones . Milestones mark specific points along your project timeline that identify when activities have been completed or when a new phase starts
Create a timeline or Gantt chart to get a better overview of your prioritized tasks, milestones, and deadlines. Your timeline also serves as a visual way to track the start and end dates of every task in your action plan. You can use it as a baseline to make sure your team stays on track.
Step 6: Monitor and revise your action plan
Your ability to stay on top of and adapt to changes is what makes you a great project manager. It’s crucial that you monitor your team’s progress and revise the plan when necessary.
Luckily, your action plan isn’t set in stone. The best way to track potentially changing priorities or deadlines is to use a dynamic tool like a work management software . That way, you can update to-dos and dependencies in real time, keep your team on the same page, and your action plan moving.
Action plan vs. plan B vs. project plan vs. to-do list
So how exactly does an action plan differ from all these other plans and lists? To clear this up once and for all, we’re going to explain what these plans are and when to use which plan to maximize your team’s efforts.
Action plan vs. plan B
You may have heard the terms action plan and plan B used interchangeably. But in fact, an action plan and plan B are two completely different types of plans. Here’s how to tell them apart:
Your action plan outlines actions in much detail so you and your team know exactly what steps to take to reach your goal.
A plan B is a secondary action plan, an alternative strategy, that your team can apply if your original plan fails. Whether that’s because of an internal issue or an external factor—having a plan B is a great way to be prepared for the worst case scenario.

Action plan vs. project plan
A project plan is a bit more complicated than an action plan. Project plans are blueprints of the key elements your team needs to accomplish to successfully achieve your project goals. A project plan includes seven elements:
Goals and project objectives
Success metrics
Stakeholders and roles
Scope and budget
Milestones and deliverables
Timeline and schedule
Communication plan
Once you’ve created a project plan, use an action plan to outline and document how your team will execute your tasks and hit your goals. This will ensure that everyone on your team knows what their responsibilities are and what to get done by when.
Action plan vs. to-do list
A to-do list is typically used to write down single tasks that don’t necessarily lead to one common goal. To-do lists can change daily and are much less organized than action plans. An action plan will follow specific steps and include tasks that all lead to the completion of a common goal.
How to implement your action plan successfully
You know how to create an action plan, but in order to implement it successfully, you need to use the right tools and use them correctly. Here are our top five tips to ensure your action plan is effective:

Use task management software
Streamline your action plan by keeping all of your tasks and timelines in one central source of truth. Task management software, like Asana , is perfect for your action plan because it allows you to keep track of pending tasks, declare task ownership, assign dependencies, and connect with your team in real time or asynchronously .
Use or create templates
Create or use a template that lists all the action items with notes, status, priority, and ownership. When you create a template that fits your project type, you can reuse it time and time again.
Set up real-time alerts and assign dependencies
Make sure all action items are time-bound and that you assign dependencies. That way, your team can react when an item is ready for them and easily track what other items depend on theirs.
Check action items off as you complete them
When action items are completed, check them off! Make sure it’s visible to everyone and happens in real time so the person responsible for the next action item can start their work as soon as possible.
Discuss late or pending tasks
If you run into issues or delays, talk to your team to uncover potential bottlenecks and find solutions that keep the action plan on track. You can add notes directly into your action plan or set up calls to discuss more complex issues.
Ready, set, action plan
Like Benjamin Franklin once said: “If you fail to plan, you are planning to fail.” Creating an action plan helps you stay focused, on track, and brings your goals to life.
Plan to succeed with a structured action plan and helpful tools like Asana’s task management software. Connect and align with your team in a central source of truth while staying flexible enough to revise your action plan when necessary.
Related resources

What's the difference between accuracy and precision?

How Asana streamlines strategic planning with work management

What is management by objectives (MBO)?

7 steps to complete a social media audit (with template)
JavaScript seems to be disabled in your browser. For the best experience on our site, be sure to turn on Javascript in your browser.
The Seven Steps of Action Planning

- Define the Problem(s)
- Collect and Analyze the Data
- Clarify and Prioritize the Problem(s)
- Write a Goal Statement for Each Solution
- Implement Solutions: The Action Plan
- Monitor and Evaluate
- Restart with a New Problem, or Refine the Old Problem
The following is a simple example of the problem solving process in practice: The dairy farm owner notices that the bulk tank weights are lower this week than last week. In the next sections we will go through the seven steps to solve this problem:
Step 1: Define the Problem(s)
Evaluate the situation. Have all possibilities been considered? In this stage, explore all possibilities, ask all involved or interested individuals for their input into identifying the problem. Is there just one problem or are there more?
Our farm owner conducts a thorough investigation in trying to determine why the bulk tank weights are down. He checks with the veterinarian to be sure there is not a contributing health factor. He also has the nutritionist evaluate the ration to be sure they are feeding at the proper level. In addition, he interviews employees who interact with the cows on a daily basis. This is what he finds:
- Standard Operating Procedures are being followed thoroughly in the milking parlor.
- Several substitute feeders found some premixes in short supply. In order to feed the milking cows they had to prepare premixes before mixing the herd rations.
- The veterinarian visits and reports the cows are in good health.
- The nutritionist evaluates the rations and finds them to be appropriate for the various production groups.
The farm owner begins to suspect the problem is a result of variation in the feed ration being fed as a result of different people mixing the feed.
Step 2: Collect and Analyze the Data
Now that we have identified the problem, we collect and analyze data to prove or disprove the assumption that our problem is a result of inconsistent ration. We analyze the situations by asking questions.
- What ingredient(s) in the computer ration is the likely problem?
- What do others (veterinarian, nutritionist, herdsman) see as the reason for the lower bulk tank weights?
- What do the feeders see? How much feed is in the alley when new feed is put out?
- What does test data indicate? Compare the sample analyses of the ration being fed, the ration being eaten by the cows, and the ration left when new feed is delivered.
In our scenario, the farm owner reviews the bulk tank weights and confirms that tank weights are down. Next he checks the cow numbers to see if perhaps these are down. Instead, he finds that cow numbers are up. As he is gathering data from the employees he is reminded that the old feeder left for a new position. He finds that different people have been pitching in to mix the feed ration. The owner begins to suspect that the cow's daily rations are not being made consistently. He reviews analysis of feed samples at the next three feedings and finds that the variation is beyond the limits for acceptability.
Step 3: Clarify and Prioritize the Problem(s)
If there is more than one problem, you will need to prioritize the problems so you can focus on the most important problems first. Ask the following questions to help you sort the problems with the higher priority issues at the top of the list.
- Which problem could result in negative consequences in terms of cow or employee health?
- Are any of the problems putting the operation in danger of being in noncompliance with regulations?
- Which problems have the greatest impact on the long-term economic stability of the operation?
- Which problems have short-term impact on the stability of the operation?
In this case we only have one problem -- lack of a consistent ration so prioritization is not necessary.
Step 4: Write a Goal Statement for Each Solution
The next step in the process is setting S.M.A.R.T. goals, or goals that are:
S - Specific
M - measurable, a - achievable, r - relevant.
The team needs to go through the problems that have been identified and evaluate them for each of these items. If all the goals that have been set are S.M.A.R.T. goals, great -- you are ready to move on to Monitoring Progress. Otherwise, work with the team to make the necessary adjustments to make the goals S.M.A.R.T.
Specific goals are clear and focused, not broad, ambiguous, or general. Specific goals provide specific information on the behaviors that are associated with the goal. These goals indicate who will do what, when and how.
- Example of a goal that is not specific - "The advisory team will improve Pleasantview Dairy's profitability."
- Example of a specific goal - "Employees of Pleasantview Dairy will lower feed costs by producing high-quality forages (RFV>125), having forage equipment in top working order by May 1, storing the first crop of hay silage by May 25, and continuing to harvest at 31-day intervals throughout the growing season."
Measurable goals provide a measurable indicator of success, so that it becomes easy to monitor progress and determine when success has been attained. Measurements of success may be quantified with numbers or a simple yes/no determination.
- Example of a goal that is not measurable - "Employees of Pleasantview Dairy will improve feed quality."
- Example of a measurable goal - "Employees of Pleasantview Dairy will increase the average relative feed value from 100 to greater than 140 for all hay silage stored this summer" or "All ingredients in the TMR will be weighed using the electronic scales and delivered to the feed bunk by 10:00 a.m."
Achievable goals are realistic, and well within the abilities, responsibilities and resources of the management and staff. This does not mean that goals must be easy to achieve. Every effort should be made to reach a higher level of performance. Sometimes "stretch" goals can encourage someone to step out of their comfort zone and tackle tasks in a new, challenging, yet achievable way that results in overall improvement for the operation.
- Example of a goal that is not achievable - "Milk yields will exceed x amount," where x is beyond the limitations for the breed of cattle, facilities and management of the operation.
- Example of an achievable goal - "Farm employee x will mix feed ingredients accurately (wet feed less than 5 percent and dry feed less than 1 percent error) and deliver it to the cows by 10:00 a.m."
A relevant goal is appropriate to a person who will be attempting to achieve it and to the overall goals and objectives of the farm.
- Example of a goal that is not relevant - "All feed will be delivered to the cows by 10:00 a.m." This goal is easy enough to measure and achieve, but doesn't do anything to ensure the quality of the feed.
- Example of a relevant goal - "Farm staff will improve milk production and lower feed waste by assuring that the computed ration is fed to the cows accurately, in the proper amounts and by 10:00 a.m. each morning."
The attainment of a goal should not be open-ended, but set for a specific time. As much as possible, the exact date the goal is to be achieved should be determined. When a goal has a deadline, it provides a measurable point and speeds progress toward critical goals. Employees will generally put more emphasis on goals that have specific deadlines than on those for which no time for measurement has been established.
- Example of a goal that is not timely - "We will increase milk sold per worker to 1.2 million pounds."
- Example of a timely goal - "We will increase milk sold per worker to 1.2 million pounds by July 1 of next year."
Now, back to our example - an appropriate S.M.A.R.T. goal for this situation would be to write a standard operating procedure (SOP) by tomorrow evening's feeding so that everyone that is assigned to feed the cows unexpectedly can easily follow the steps and assure that the cows are fed correctly twice daily, at 6 a.m. and 6 p.m.
Step 5: Implement Solutions - The Action Plan
Step five is to write an action plan that addresses the problems. An action plan is written so that any employee can do the task successfully alone and is followed much like a recipe. It converts the goal or plan into a people process. It has three essential parts:
- Based on the goal the action plans answers five questions - What? When? How? Where? Who?
- Lists Resources
- Lists Potential Barriers
The example below applies these steps to our sample problem. Some of the steps in the action plan are obvious.
- What? - Feed the cows correctly twice a day.
- When? - By tomorrow night.
- How? - The written SOP.
Some questions still need answers in the action plan
- Where? - Feed is to be mixed in the feed wagon using the green tractor on the concrete pad by the commodity bins next to the silos. The feed is then to be fed to the cows in lots 2, 3, and 4 twice daily, at 6AM and 6 PM.
- Who? - To be assigned by the herdsman until a new feeder is hired and trained.
Resource List
- Ask the herdsman for help if any questions arise.
- The feeds are in the feed storage area and will be replaced as they are used.
- The tractor and mixing wagon are in the shed by the feed storage.
- The feeder is authorized to order feed or ask the office to do so.
- The feeder can spend up to $300 to correct problems when the office is closed and should get parts on account at Dickerson's Equipment.
Potential Barriers
- Depleted feeds in silos or bins.
- Tractor is in use somewhere else.
- Broken equipment.
- Sick employees.
- Cows in the wrong lot.
- Scales broken.
You will want to post an alternative plan for each of these contingencies.
Step 6: Monitor and Evaluate
Our next step in the problem solving process is to design a method for monitoring the outcome. The method we select should assess whether the goal and action plan corrects the problem. In addition, a well-designed monitoring method will help the team to determine when the action plan needs to be improved.
A team of professionals should not spend much time going over numerous data sets. They should have simple spreadsheets or graphs that tell how well the action plan is working and move on to bigger problems. Most teams need a short list of key parameters related to goals that they follow each meeting. An extensive list of production items is provided in the Resource/Special Tools section for ideas. Many teams track summary data from accounting reports, inventories of resources, or other items critical to monitoring action plans.
At each team meeting, the team should receive an update on the progress towards meeting the goals including any difficulties encountered or benefits received. Printed reports, summaries and spreadsheets speed the work of the team and help track progress. As time passes and situations change, the team will need to reevaluate individual goals and action steps as well as eliminate any that are no longer necessary. Add new goals as the need arises.
In our example, there were several components of the monitoring and evaluation process.
- Grab samples were taken and analyzed at each feeding for the next two weeks.
- The herdsman routinely observed the feed mixing process to see that the standard operating procedure was being followed.
- Bulk tank weights were monitored and plotted with cow numbers on a graph on a wall in the parlor office.
Monitoring Tools: Sample Herd Report
Step 7: Restart With a New Problem, or Refine the Old Problem
The problem solving steps are cyclical. If the first cycle is successful the process starts over with a new problem. If the same problem persists, there must be refinement, so the process starts over with refinement of the original problem as more current data is analyzed.
The problem solving process can last minutes or extend to years depending on the difficulty and complexity of the problem being addressed. Some problems will be addressed "on the fly" by the farm owner. Others will require careful consideration by the farm advisory team.

- Dairy Advisory Teams
- Integrated Dairy Management
You may also be interested in ...

Milk Production Records for Management Control

Feeding Records for Management Control

Standard Operating Procedures: A Writing Guide

Heifer Economics

Economics and Effects of Accelerated Calf Growth Programs

Dairy Sense: Keeping the Dairy Right Sized

Dairy Cropping System Project – Forage Quality and Quantity, Part I

Using Quickbooks to Manage Your Farm Business

Using QuickBooks to Manage Your Farm Business: Instructor-Guided

Evaluating and Conditioning Cull Cattle for Market
Personalize your experience with penn state extension and stay informed of the latest in agriculture..
Search form

- Table of Contents
- Troubleshooting Guide
- A Model for Getting Started
- Justice Action Toolkit
- Best Change Processes
- Databases of Best Practices
- Online Courses
- Ask an Advisor
- Subscribe to eNewsletter
- Community Stories
- YouTube Channel
- About the Tool Box
- How to Use the Tool Box
- Privacy Statement
- Workstation/Check Box Sign-In
- Online Training Courses
- Capacity Building Training
- Training Curriculum - Order Now
- Community Check Box Evaluation System
- Build Your Toolbox
- Facilitation of Community Processes
- Community Health Assessment and Planning
- Section 5. Developing an Action Plan
Chapter 8 Sections
- Section 1. An Overview of Strategic Planning or "VMOSA" (Vision, Mission, Objectives, Strategies, and Action Plans)
- Section 2. Proclaiming Your Dream: Developing Vision and Mission Statements
- Section 3. Creating Objectives
- Section 4. Developing Successful Strategies
- Section 6. Obtaining Feedback from Constituents: What Changes are Important and Feasible?
- Section 7. Identifying Action Steps in Bringing About Community and System Change
|
The Tool Box needs your help Your contribution can help change lives.
|
|
Sixteen training modules
|
- Main Section
| Learn how to make your vision concrete by describing the strategies that your organization will use to meet its goals and objectives. |

Developing an action plan can help changemakers turn their visions into reality, and increase efficiency and accountability within an organization. An action plan describes the way your organization will meet its objectives through detailed action steps that describe how and when these steps will be taken. This section provides a guide for developing and utilizing your group's action plan.
What is an action plan?
In some ways, an action plan is a "heroic" act: it helps us turn our dreams into a reality. An action plan is a way to make sure your organization's vision is made concrete. It describes the way your group will use its strategies to meet its objectives. An action plan consists of a number of action steps or changes to be brought about in your community.
Each action step or change to be sought should include the following information:
- What actions or changes will occur
- Who will carry out these changes
- By when they will take place, and for how long
- What resources (i.e., money, staff) are needed to carry out these changes
- Communication (who should know what?)
What are the criteria for a good action plan?
The action plan for your initiative should meet several criteria.
Is the action plan:
- Complete ? Does it list all the action steps or changes to be sought in all relevant parts of the community (e.g., schools, business, government, faith community)?
- Clear ? Is it apparent who will do what by when?
- Current ? Does the action plan reflect the current work? Does it anticipate newly emerging opportunities and barriers?
Why should you develop an action plan?
There is an inspirational adage that says, "People don't plan to fail. Instead they fail to plan." Because you certainly don't want to fail, it makes sense to take all of the steps necessary to ensure success, including developing an action plan.
There are lots of good reasons to work out the details of your organization's work in an action plan, including:
- To lend credibility to your organization. An action plan shows members of the community (including grantmakers) that your organization is well ordered and dedicated to getting things done.
- To be sure you don't overlook any of the details
- To understand what is and isn't possible for your organization to do
- For efficiency: to save time, energy, and resources in the long run
- For accountability: To increase the chances that people will do what needs to be done
When should you create an action plan?
Ideally, an action plan should be developed within the first six months to one year of the start of an organization. It is developed after you have determined the vision, mission, objectives, and strategies of your group. If you develop an action plan when you are ready to start getting things done, it will give you a blueprint for running your organization or initiative.
Remember, though, that an action plan is always a work in progress. It is not something you can write, lock in your file drawers, and forget about. Keep it visible. Display it prominently. As your organization changes and grows, you will want to continually (usually monthly) revise your action plan to fit the changing needs of your group and community.
How to write an action plan
Determine what people and sectors of the community should be changed and involved in finding solutions.
If you have been using the VMOSA (Vision, Mission, Objectives, Strategies, Action Plans) model, you might have already done this, when you were deciding upon your group's objectives. Again, try to be inclusive. Most of the health and development issues that community partnerships deal with are community-wide, and thus need a community-wide solution. Possible sectors include the media, the business community, religious organizations, schools, youth organizations, social service organizations, health organizations, and others.
Some members of the community you might consider asking to join the action planning group include:
- Influential people from all the parts of the community affected by your initiative (e.g., from churches and synagogues, the school system, law enforcement, etc.)
- People who are directly involved in the problem (e.g., local high school students and their parents might be involved in planning a coalition trying to reduce teen substance use)
- Members of grassroots organizations
- Members of the various ethnic and cultural groups in your community
- People you know who are interested in the problem or issue
- Newcomers or young people in the community who are not yet involved
Let's consider some of the people who were involved with the planning group for the fictional Reducing the Risks (RTR) Coalition that hopes to reduce the rate of teen pregnancy. Some of the members of this planning group included teachers at the local high school, local teenagers and their parents, members of the clergy, counselors and school nurses, staff of the county health department, and members of youth organizations, service agencies, and other organizations that focus on youth issues.
Convene a planning group in your community to design your action plan . This might be the same group of people who worked with you to decide your group's strategies and objectives. If you are organizing a new group of people, try to make your planning committee as diverse and inclusive as possible. Your group should look like the people most affected by the problem or issue.
Once everyone is present, go over your organization's:
- Targets and agents of change (e.g., youth, parents and guardians, clergy)
- Proposed changes for each sector of the community (e.g., schools, faith community, service organizations, health organizations, government)
Develop an action plan composed of action steps that address all proposed changes. The plan should be complete, clear, and current. Additionally, the action plan should include information and ideas you have already gathered while brainstorming about your objectives and your strategies. What are the steps you must take to carry out your objectives while still fulfilling your vision and mission? Now it's time for all of the VMOSA components to come together. While the plan might address general goals you want to see accomplished, the action steps will help you determine the specific actions you will take to help make your vision a reality. Here are some guidelines to follow to write action steps.
Members of the community initiative will want to determine:
- What action or change will occur
- Who will carry it out
- When it will take place, and for how long
- What resources (i.e., money, staff) are needed to carry out the change
- Communication (who should know what)
Example: RTR Coalition's Action Step (a sample) One community change sought by this coalition to prevent teen pregnancy was to increase publicity about contraception and unwanted pregnancy at the local high school. What action or change will occur: Hanging posters, displays, and other information about contraception and the facts about unwanted pregnancy in the hallways of the local high school. The posters and other information will become a permanent part of the high school. Posters and information will be regularly changed as new materials become available. Who will carry it out: A sub-committee comprised of parents and guardians, teachers, students, and coalition members will be responsible for maintaining the displays. The coalition as a whole will work towards finding funding to purchase the materials. Maria and Alex of the schools action group will be responsible for researching and ordering the materials. By when will it take place, and for how long: The coalition will try to have posters hanging and displays visible within six weeks of deciding on the action step (2/19/2013). What resources are needed to carry out the step: The coalition will approach the school district to request funding for the project. Otherwise, the group will seek funding from other sources such as foundations and local businesses to finance the program. Communication about the action step. The school principal and leadership of the Parent-Teacher Organization (PTO) should be given information about this planned change.
Things to note about this portion of the RTR action plan:
- It appears complete . Although this step seems fully developed, we would need to review the entire action plan to see whether all community and system changes that should be sought are included.
- It is clear . We know who will do what by when.
- It seems current . We would need to know more about other current work (and new opportunities and barriers) to judge whether this portion of the action plan is up-to-date.
Review your completed action plan carefully to check for completeness. Make sure that each proposed change will help accomplish your group's mission. Also, be sure that the action plan taken as a whole will help you complete your mission; that is, make sure you aren't leaving anything out.
Follow through. One hard part (figuring out what to do) is finished. Now take your plan and run with it! Remember the 80-20 rule: successful efforts are 80% follow through on planned actions and 20% planning for success.
Keep everyone informed about what's going on. Communicate to everyone involved how his or her input was incorporated. No one likes to feel like her wit and wisdom has been ignored.
Keep track of what (and how well) you've done. Always keep track of what the group has actually done. If the community change (a new program or policy) took significant time or resources, it's also a good idea to evaluate what you have done, either formally or informally.
Keep several questions in mind for both yourself and others:
- Are we doing what we said we'd do?
- Are we doing it well?
- Is what we are doing advancing the mission?
You can address these questions informally (ask yourself, chat with friends and other people), as well as formally, through surveys and other evaluation methods.
Celebrate a job well done! Celebrate your accomplishments; you and those you work with deserve it. Celebration helps keep everyone excited and interested in the work they are doing.
After you've written your action plan: Getting members to do what they said they would
Every community organization has undoubtedly had this happen: you plan and you assign tasks to get everything you've planned to do accomplished. Everyone agrees (maybe they even offer) to do certain tasks, and you all leave with a great feeling of accomplishment. The problem? At the next meeting, nothing has been done. Besides tearing out your hair, what can you do?
Fortunately, there are several things you can try. It's particularly tricky in the case of volunteers, because you don't want to lean too hard on someone who is donating their time and energy to begin with. Still, you can make it easier for members to get things done (and harder to avoid work) without acting like the mean neighbor down the street. Some of these gentle reminders include:
- Regular phone calls from staff members or dedicated volunteers asking others how they are doing with their tasks. This should be a supportive call, not a "are you doing what you're supposed to" call. The person calling can offer emotional support "how are you doing?" as well as see if the group member needs any other assistance. A friendly call such as this can be seen as helpful, give the member the sense that he is a very important part of the group, and serve as a great reminder to do what he said he would do.
- Distributing the action plan in writing to all members, with names attached to specific tasks. (Additionally, this can be a great time to ask for feedback before the plan becomes "official.")
- Making sure timelines (with due dates) are complete, clear and current.
- At regular group meetings, such as committee meetings or board meetings, ask members to report on accomplishing the tasks they have set out to do. Consider making this a regular part of the meeting.
- Celebrate the accomplishment of tasks. It's important that getting something done actually means something, and is recognized by the group as a whole.
Follow up on the action plan regularly. You are asking members to be accountable, and to get things done on a regular basis. If they have agreed, you should help them fulfill their commitment as best you can.
Online Resources
The Ruckus Society offers an Action Planning Manual that discusses strategies for nonviolent direct action.
Preventing Adolescent Substance Abuse: An Action Planning Guide for Community-Based Initiatives
Preventing Youth Violence: An Action Planning Guide for Community-Based Initiatives
Preventing Adolescent Pregnancy: An Action Planning Guide for Community-Based Initiatives
Promoting Child Well-Being: An Action Planning Guide for Community-Based Initiatives
Promoting Urban Neighborhood Development: An Action Planning Guide for Improving Housing, Jobs, Education, Safety and Health
Preventing Child Abuse and Neglect : An Action Planning Guide for Community-Based Initiatives
Reducing Risk for Chronic Disease: An Action Planning Guide for Community-Based Initiatives
Print Resources
Barry, B. (1984). Strategic planning workbook for nonprofit organizations . St. Paul: MN: Amherst H. Wilder Foundation.
Berkowitz, W. (1982). Community impact: creating grassroots change in hard times . Cambridge, MA: Schenkman Publishing.
Bryson, J. (1988). Strategic planning for public and nonprofit organizations: A guide to strengthening and sustaining organizational achievement . San Francisco: Jossey-Bass Publishers.
Fawcett, S., Paine, A., Francisco, V., Richter, K., Lewis, R., Williams, E., Harris, K., Winter, K., in collaboration with Bradley, B. & Copple, J. (1992). Preventing adolescent substance abuse: an action planning guide for community-based initiatives . Lawrence, KS: Work Group on Health Promotion and Community Development, University of Kansas.
Fawcett, S., Claassen, L., Thurman, T., Whitney, H., & Cheng, H. (1996). Preventing child abuse and neglect: an action planning guide for building a caring community . Lawrence, KS: Work Group on Health Promotion and Community Development, University of Kansas.
Kansas Health Foundation. VMOSA: An approach to strategic planning . Wichita, KS: Kansas Health Foundation.
Lord, R. (1989). The nonprofit problem solver . New York, NY: Praeger.
Olenick, A. & Olenick, P. (1991). A nonprofit organization manual . New York, NY: The Foundation Center.
Unterman, I., & Davis, R. (1984). Strategic management of not-for-profit organizations . New York, NY: CBS Educational and Professional Publishing.
Wolf, T. (1990). Managing a nonprofit organization . New York, NY: Prentice Hall.
Watson-Thompson, J., Fawcett, S., & Schultz, J. (2008). Differential effects of strategic planning on community change in two urban neighborhood coalitions. American Journal of Community Psychology, 42, 25-38.
Alternative Courses of Action in Case Study: Examples and How To Write

The ultimate goal of creating a case study is to develop a feasible action that can solve the problem it raised.
One way to achieve this is by enumerating all the possible solutions for your case study’s subject. The portion of the case study where you perform this is called ACA or Alternative Courses of Action.
Are you struggling with writing your case study’s ACA? Do not worry; we have provided you with the most detailed guide on writing the Alternative Courses of Action (ACA) of a case study.
Table of Contents
What are alternative courses of action (aca) in a case study.
Alternative Courses of Action (ACA) are the possible actions a firm or organization can implement to address the problem indicated in the case study. These are suggested actions that a firm can consider to arrive at the most feasible and effective solution to the problem.
This portion doesn’t provide the actual and optimal solution yet. Instead, it contains proposed alternatives that will still undergo an evaluation of their respective advantages and disadvantages to help you come up with the best solution.
The ACA you will offer and indicate will be based on your case study’s SWOT analysis in the “ Areas of Consideration ” portion. Thus, a SWOT analysis is performed first before writing the ACA.
What Is the Importance of Alternative Courses of Action (ACA) in a Case Study?
Given the financial, logistical, and operational limitations, developing solutions that the firm can perform can be challenging. By enumerating and evaluating the ACA of your case study, you can filter out the alternatives that can be a potential solution to the problem, given the business’s constraints 1 . This makes your proposed solutions feasible and more meaningful.
How To Write Alternative Courses of Action in Case Study
Here are the steps on how to write the Alternative Courses of Action for your case study:
1. Analyze the Results of Your SWOT Analysis

Using the SWOT analysis, consider how the firm can use its strengths and opportunities to address its weaknesses, mitigate threats, and eventually solve the case study’s problem.
Suppose that the case study’s problem is declining monthly sales, and the SWOT analysis showed the following:
- Strength : Creative marketing team
- Opportunity : Increasing trend of using social media to promote products
Then, you may include an ACA about developing the digital marketing arm of the firm to attract more customers and boost monthly sales. This can also address one of the possible threats the firm faces, which is increasing direct marketing costs.
2. Write Your Proposed Solutions/Alternative Courses of Action (ACA) for Your Case Study’s Problem

Once you have reviewed your SWOT analysis and come up with possible solutions, it’s time to write them formally in your manuscript. Each solution does not have to be too detailed and wordy. State the specific action that the firm must perform concisely.
Going back to our previous example in Step 1, here is one of the possible ACA that can be included:
ACA #1: Utilize digital platforms such as web pages and social media sites as an alternative marketing platform to reach a wider potential customer base. Digital marketing, together with the traditional direct marketing strategy currently employed, maximizes the business’ market presence, attracting more customers, and potentially driving revenues upward.
In our example above, there is a clear statement of the firm’s action: to use web pages and social media sites to reach more potential customers and increase market presence. Notice how the ACA above provides only an overview of “what to do” and not a complete elaboration on “how to do it.”
3. Identify the Advantages and Disadvantages of Each ACA You Have Proposed

After specifying the ACA, you must evaluate them by stating their respective advantages (pros) and disadvantages (cons). In other words, you must state how your ACA favors the firm (advantages) and its downsides and limitations (disadvantages).
Again, your evaluation does not have to be too detailed but make sure that it is relevant to the ACA that it pertains to.
Let’s return to the ACA we developed from step 2, utilizing digital platforms (e.g., social media sites) to reach more potential customers. What do you think will be the pros and cons of this ACA?
Let’s start with its potential benefits (advantages). Using digital platforms is cheaper than using print ads or direct marketing. So, this will save some funds for the firm. In short, it is cost-effective.
Second, digital platforms offer analytical tools to measure your ads’ reach, making it easier to evaluate people’s perceptions of your offering.
Third, using social media sites makes communicating with any potential customer easier. You can quickly respond to their queries, especially if they are interested in your product.
Lastly, you can reach as many types of people as possible by taking advantage of the internet algorithm.
Now, let us consider its disadvantages 2 . First, using digital marketing takes time and effort to learn, and you must be able to adapt quickly to the changes in trends and new strategies to keep up with the competition.
Second, you must deal with the increasing market competition, as many businesses already use digital platforms.
Third, you have to deal with negative feedback from your customers that are visible to the public and may affect their perception of your brand.
After pondering over the pros and cons of your ACA, it’s time to write them concisely in your manuscript. You can present it in two ways: by tabulating it or by simply listing them.
Example in Table Form:
| | – Cost-effective – Provide analytical tools to evaluate ad reach and performance – A more accessible and more convenient platform to communicate with potential customers and address their queries and concerns – Maximize reach to potential customers anywhere – Time-consuming and challenging to learn due to changes in trends and strategies – Increasing market competition as many businesses also use digital platforms. – Negative feedback reflected in the digital platform could affect people’s perception of the firm |
Examples of Alternative Courses of Action (ACA) in a Case Study
Case Study Problem: Xenon Pastries faces a problem handling larger orders as Christmas Day approaches. With an estimated 15% increase in customer demand, this is the most significant increase in their daily orders since 2012. The management aims to maximize profit opportunities given the rise in customer demand.
ACA #1: Hire part-time workers to increase staff numbers and meet the overwhelming seasonal increase in customer orders. Currently, Xenon Pastries has a total of 9 workers who are responsible for the accommodation of orders, preparation, and delivery of products, and addressing customers’ inquiries and complaints. Hiring 2 – 3 part-time workers can increase productivity and meet the daily order volume.
- Do not require too much effort to implement since hiring announcements only require signages or social media postings
- High certainty of finding potential workers due to the high unemployment rate
- Improve overall productivity of the business and the well-being of other workers since their workload will be lessened
Disadvantages
- Increase in operating expense in the form of wages to the new workers
- Managing more employees and monitoring their performance can be challenging
- New workers might find it challenging to adapt essential skills required in the operation of the business
ACA #2: Increase the prices of Xenon pastries’ products to increase revenues . This option can maximize Xenon Pastries’ profit even if not all customers’ orders are accommodated.
- Cost-effective
- Easy to implement since it only requires changing the price tags of the products
- If customers’ desire to buy the products does not change, the price increase will certainly increase the business’ revenue
- Some customers might be discouraged from buying because of an increase in prices
- There’s a possibility that the increase in the price of the products will make it more expensive relative to competitors’ products
Case Study Problem: Delta Motors has been manufacturing motorcycles for ten years. Recently, the business suffered a gradual shrink in its quarterly revenues due to the increasing popularity of traditional and newly-developed electric bikes. Delta Motors seeks a long-term strategy to attract potential customers to bounce back sales.
ACA #1: Develop a “regular installment payment” scheme to attract customers who wish to purchase motorcycles but have insufficient lump-sum money to acquire one. This payment scheme allows customers to pay an initial deposit and the remaining amount through smaller monthly payments.
- Enticing for middle to low-income individuals who comprise a large chunk of the population
- Requires low initial capital to implement
- Provides a new source of monthly income streams that can benefit the financial standing of the company
- Risk of default or delays in installment payments
- Requires additional human resources to manage and collect installment payments
- The payment scheme requires time to gain returns due to the periodic flow of funds
- Requires a careful creation of guidelines and terms and conditions to ensure smooth facilitation of the installment payment scheme
ACA #2: Introduce new motorcycle models that can entice different types of customers. These models will feature popular designs and more efficient engines.
- This may capture the public’s interest in Delta Motors, which can lead to an increase in the number of potential customers and earning opportunities
- Enables the business to keep up with the intense market competition by providing something “fresh” to the public
- Provides more alternatives for those who already support Delta Motors, strengthening their loyalty to the brand
- Conceptualization of a new model takes a lot of brainstorming to test its feasibility and effectiveness
- Requires sufficient funds to sustain the investment for the development of a new model
- It requires effective marketing strategies to promote the new model to the public
Tips and Warnings
- Do not include in this portion your case study’s conclusion . Think of ACA as a list of possible ways to address the problem. In other words, you suggest the possible alternatives to be selected here. The “ Recommendation ” portion of your case study is where you pick the most appropriate way to solve the problem.
- Use statistical data to support the advantages and disadvantages of each ACA. Although this is optional, presenting numerical data makes your analysis more concrete and factual than just stating them descriptively.
- Do not fall into the “meat sandwich” trap. This happens when you intently make some of the alternatives less desirable so that your preferred choice stands out. This can be done by refusing to elaborate on their benefits or excessively concentrating on their disadvantages. Make sure that each ACA has potential and can be implemented realistically.
Frequently Asked Questions
1. how many alternative courses of action (aca) can a case study have.
Sometimes your instructor or teacher will tell you the required number of ACA that must be included in your case study . However, there’s no “standard” limit to how many ACA you can indicate.
2. What is the difference between Alternative Courses of Action (ACA) and Recommendations?
As mentioned earlier, the case study’s ACA aims to enumerate all possible solutions to the problem. It is not the stage where you state the “final” action you deem most appropriate to address the issue. The case study portion where you explicitly mention your “best” alternative is called the “Recommendation.”
To help you understand the point above, let’s return to our Delta Motors example. In our previous section, we have provided two ACA that can solve the problem, namely (1) developing a regular installment payment plan and (2) introducing a new motorcycle model.
Suppose that upon careful analysis and evaluation of these ACA, you came up with ACA #2 as the more fitting solution to the problem. When you write your case study’s recommendation, you must indicate the ACA you chose and your reasons for selecting it.
Here’s an example of the Recommendation of the case study:
Recommendation
Introducing new motorcycle models that feature popular designs and more efficient engines to entice different types of customers is the most promising alternative course of action that Delta Motors can implement to bounce back its quarterly revenues and keep up with the competitive market. This creates a strong impression on the public of the company’s dedication to promoting high-quality motorcycles that can withstand changes in consumer preferences and market trends. Furthermore, this action proves that the company is continuously evolving to offer a variety of alternative models to suit everyone’s tastes. With proper promotion, these models can rekindle the company’s popularity in the automotive and motorcycle industry.
- How to Analyze a Case Study. Retrieved 23 May 2022, from https://wps.prenhall.com/bp_laudon_essbus_7/48/12303/3149605.cw/content/index.html
- Develop a Digital Marketing Plan. Retrieved 23 May 2022, from https://www.nibusinessinfo.co.uk/content/advantages-and-disadvantages-digital-marketing
Written by Jewel Kyle Fabula
in Career and Education , Juander How

Jewel Kyle Fabula
Jewel Kyle Fabula is a Bachelor of Science in Economics student at the University of the Philippines Diliman. His passion for learning mathematics developed as he competed in some mathematics competitions during his Junior High School years. He loves cats, playing video games, and listening to music.
Browse all articles written by Jewel Kyle Fabula
Copyright Notice
All materials contained on this site are protected by the Republic of the Philippines copyright law and may not be reproduced, distributed, transmitted, displayed, published, or broadcast without the prior written permission of filipiknow.net or in the case of third party materials, the owner of that content. You may not alter or remove any trademark, copyright, or other notice from copies of the content. Be warned that we have already reported and helped terminate several websites and YouTube channels for blatantly stealing our content. If you wish to use filipiknow.net content for commercial purposes, such as for content syndication, etc., please contact us at legal(at)filipiknow(dot)net
- Design for Business
- Most Recent
- Presentations
- Infographics
- Data Visualizations
- Forms and Surveys
- Video & Animation
- Case Studies
- Digital Marketing
- Design Inspiration
- Visual Thinking
- Product Updates
- Visme Webinars
- Artificial Intelligence
How to Create an Effective Action Plan (Examples & Templates)

Written by: Raja Mandal
Since you're here, you might be struggling to achieve your personal, professional or company goals. And if you think an action plan is just what you need to help you create a clear path for reaching your goals, you're absolutely right!
An effective action plan is critical, whether sending out weekly email newsletters, putting together a presentation, or executing a marketing plan or business plan . However, creating an action plan from scratch can be even more troublesome if you don’t know how to do it.
Fortunately, with Visme’s action plan templates , anyone can create an effective action plan in minutes.
Continue reading to discover what exactly an action plan is, why you need one, how to create one and some template examples that you can use it for inspiration.
Table of Contents
What is an action plan and why do you need one, why do you need an action plan, how to create an effective action plan.
10 Action Plan Templates To Help You Execute Projects
As the name suggests, an action plan is the set of tasks or activities you need to complete to achieve a goal or complete a project. You can think of it as a timeline, a list of actionable steps, people responsible for each of them and who follows the progress of each step to come up with the best results.
This single document can help you plan and monitor activities, identify the resources needed, and how and when they should be used to ultimately achieve your stated goal.
Now, you might be wondering the difference between an action plan and a to-do list. The most significant difference between these two is that to-do lists are ongoing and include tasks for different goals and projects. On the flip side, an action plan is focused on a specific goal within a limited time frame.
The purpose of creating an action plan:
- Consumer Complaint Investigation
- Project Management
- Risk and Opportunity Management
- Product Launch
- Daily Meetings
- Market Research
According to a recent study, those who finish their business plan are twice as likely to succeed in their business than those who have no business plan. So, plan to be prepared for the obstacles ahead and keep yourself on track.
And an effective action plan helps you boost your productivity and keep yourself focused. Here are some of the reasons why you need an action plan.
Get a Clear Direction
An action plan highlights the steps you should take and the timeframe to complete them. Therefore, you will get a clear direction of what to do in order to achieve your goals. So, whenever you stress yourself about the next steps or the actions taken in the past, you have everything in hand.
Keep Everyone On the Same Track
An effective action plan can bring every team member or stakeholder on the same page. It can be an individual who is an expert in the area of work, the one who is experiencing the problem and stands to benefit from the change, or who can contribute towards the goal or project.
Get a Better Clarification of the Timeframe
Every action in your action plan should have an exact completion date. Once you assign all the tasks that need to be done to achieve your goal and understand the requirements of resources for it, you can quickly figure out how long the overall action plan will take.
Measure Your Success
Measuring the success of the progress of your goal is another crucial benefit of using an action plan. For example, if an objective is to write an action plan, there may be many steps towards that goal, including understanding the design process, writing the text, branding and many others.
You can measure each of these steps to ensure you achieve the goals and contribute to the larger objective of creating an action plan.
Learning to create an action plan might seem daunting at first, but it’s worth the effort to keep yourself productive towards the goal later on. Though there is no universal formula to create an action plan, and they may differ in terms of tasks and timelines, you can follow the simple steps below to create one.
Define S.M.A.R.T. Goals
The most important ingredients you need to create an effective action plan are the goals you want to achieve. Since you are reading this, you might have already defined goals. But, if you haven’t, use the SMART method to create specific, measurable, attainable, relevant and time-bound goals.
Use the infographic below to understand a SMART goal and try to create yours accordingly.

Once you have set SMART goals, you are already halfway through achieving them. If you struggle with creating SMART goals, use the worksheet template below.

Additionally, read the article on how to create SMART goals to learn more about it.
Prepare the List of Actions
Now, prepare a list of actions you need to take to reach your goal. It would be better to divide your main goal into smaller actionable steps to make the final goal less overwhelming and get closer to achieving your goal one step at a time.
However, make sure that the actions are realistic and relevant to your goal. For example, if you want to generate 30% more leads, some of your actions could be creating engaging content, optimizing your web pages, asking for referrals, and many others.
Identify and Allocate Resources
Before creating the action plan, you must identify all the resources required to complete the tasks. Some of the resources you need will include money, equipment, personnel, tools and others. And if you don’t have the resources available at the moment, you need to make a plan to acquire them.
Once you have your resources, allocate them to the right people. For example, suppose you are running a digital marketing campaign. In that case, you will need to have the applications and tools for content production, graphic design, and marketing analytics and hand them over to your content manager, social media manager and SEO manager.
Set the Deadline
As we have already discussed, the goals should be SMART. And here, T stands for time-bound, which means that you should have a start and finish date to achieve your goal. If you don’t do it, you are likely to never reach the goal.
Therefore, choose a specific deadline so the other team members involved can plan better for the execution of the action plan.
Additionally, you can break one large goal into smaller subgoals and set an individual deadline for each of them. For example, if you want to generate 30% more leads by the end of Q4 this year, you can set subgoals such as:
- Upload first YouTube video by X date.
- Publish 250 blog posts by X date.
- Host 25 webinars by X date.
Create a Visual Representation
Now, let’s move to the part where you will actually materialize your action plan. Creating a visual representation of the action plan is the best way to engage your team so that everyone knows the plan well.
But designing an action plan from scratch is not an easy task. Visme is there to help you design the action plan without stressing yourself out for the design part. Follow the steps below to visualize your action plan.
Pick a Template
Visme offers a wide range of professionally designed action plan templates for various business types and use cases. Choose a template from the library that suits your needs or that you can easily customize a little to create your very own action plan.
Input Your Text and Data
Now, edit the empty fields to fill in your objectives, tasks, deadline, budget, and many others. Click on one of the text boxes and start typing to insert your text or replace any pre-existing text with your own.
Change the Colors and Fonts
Customize the appearance of your action plan further by changing the colors and fonts. Select the element you want to change color for and use the color picker tool to change the color according to your need.
Once you are done with the colors, you can now change the font style, color and size. Double click on the text that you want to change the font for and use the editor on top to do it.
Use your brand colors and brand fonts in the action plan to perfectly represent your brand. Visme lets you save your brand assets so that you get customized templates according to your brand guidelines at your fingertips.
Watch the video below to learn more about setting up your brand identity kit in Visme.

Incorporate Icons and Illustrations
Icons and illustrations are the essential part of visually expressing actions and ideas. Add relevant icons and illustrations or swap out the ones included to ensure they match your action plan. Visme offers thousands of professionally crafted icons and illustrations that you can use in your design.
Additionally, take your design to the next level effortlessly by incorporating 3D animated assets in your action plan.
Collaborate with Your Team
To make the most of your action plan, ensure that you include all the team members that you think can contribute to the success of your plan. Start collaborating with your team and effectively create stunning designs right inside Visme.
Check out the video tutorial below to learn more about it.

Share Your Action Plan
Once you are satisfied with your action plan, you can share it with your team members. Download the action plan as a high-resolution JPG or PNG image file or share it via a link. If you want to publish your action plan on a website to blog, generate an embedded link and paste it wherever you want.
Monitor the Progress
Track your progress regularly and ensure that each step in your action plan is completed on time. You can use an internal reporting system or hold regular meetings to track progress. Mark tasks that are completed as done on the action plan to bring them to the attention of your team members.
This will help you better understand the pending or delayed tasks for which you need to find solutions. Finally, keep updating the action plan regularly according to your progress. With Dynamic Fields , it's easy to keep your action plan, and all other projects, updated. Once you input data into a dynamic field, it will change across all projects it’s used in.
If you are considering the action plan for a project, you can also opt for project management plan templates to keep track of your project progress and ensure a smooth operation.
Additionally, Visme offers a wide variety of other documents such as status reports , marketing plans , sales plans , project plans , organizational charts and many more.
10 Action Plan Templates to Help You Execute Projects
1. marketing action plan.
Planning marketing and promotional activities are critical aspects of your business process as they help you achieve your business goals and grow your business. If you are a marketer, you should plan activities each month and compare them with your expected results.
This action plan template can help you track the actual results of those activities and help you with your future plans. Whether your marketing objective is increasing sales or brand awareness , you can use this template as a part of your overall marketing plan .

2. 90-Day Action Plan
The position of C.E.O. comes with high expectations. With the unknowns of a new role in a new organization, the pressure to perform and the need to be accepted as a new leader by the team, it can be challenging to know where to start.
Use this 90-day action plan to understand your new organization, its target market, functional interdependencies, growth opportunities, and much more.

3. Employee Corrective Action Plan
As a business owner, you need to take corrective actions when the goals and objectives are not in line with your expectations and the process starts experiencing flaws. An employee corrective action plan is one of the crucial ones of them.
This often happens when the employee lacks key skills or doesn’t understand your organizational processes or objectives. An employee corrective action plan template like the one below allows you to record the disciplinary action that needs to be taken and suggest improvements and comments.

4. Project Action Plan
When starting or running a new project like website designing or anything else, you need to juggle many things at once. Use this website design project action plan to ensure that the project goes more smoothly.
It gives you complete visibility of the objectives, tasks and the given timeframe, making it easier for you to organize teams, assign tasks, track performance and measure the execution of the project.
Additionally, learn more about how Visme can help you better manage projects .

5. S.M.A.R.T Action Plan
You might already know that SMART goals push you further, giv1425287609es you a sense of direction and help you organize and reach your goals. Imagine what will happen if you combine your SMART goals with the action plan. Every action you take will be completely aligned with the specific goal.
This action plan template helps you do just that. Edit this template and add your SMART goal and the action steps altogether.

6. Emergency Action Plan
As a business owner, you must always be prepared for emergencies while running the business. These emergencies include hazardous materials spills, fires, natural disasters, and many others. The most effective way of handling a crisis situation is to prepare in advance by creating an emergency action plan.
The emergency action plan template helps you prepare the evacuation plan for your workplace in the event of a natural disaster. Edit this template or use it as is to do as much as possible to keep your employees safe in case of disaster.

7. Disciplinary Action Plan
The goal of a disciplinary action plan is to warn employees about what is and is not acceptable behavior in the workplace. This is mainly provided to employees during the onboarding process, but you can also use it for existing employees.
Edit this template by filling out the empty spaces with the necessary information and hand it over to the employee you want to warn of unacceptable behavior.

8. 30-60-90 Day Action Plan
The 30 60 90 day action plan is a structured way of enlisting goals and strategies in 3 steps timeline. Project managers, new hires, sales executives, and many other professionals can use this template to plan the company’s objectives and ensure that the goals are met.
This action plan template includes a 90-day action plan for a tech project split into three parts. The first 30 days show the initial steps, such as discussing project breakdown and planning with clients. Similarly, the next 60 and 90 days include other crucial actions such as quality assurance, bug fixes, feature rollout, final launch, KPI tracking, updates and many more.

9. 30-Day Action Plan
Like the 30-60-90 day action plan, the 30-day action plan is a set of steps that you need to take within 30 days to achieve the specific goal. If the project is going to take not more than 30 days or if you want to finish the project in 30 days, this action plan template is perfect for you.
This action plan template also lets you break down the project into three smaller parts to make the actions more realistic and effective. Edit this template to create the perfect 30-day action plan for any type of project you want.

10. Sales Action Plan
Create a colorful sales action plan using this template. It will help you explain how you will operate and manage the sales process to skyrocket your sales. Set goals to manage your inventory, project sales, expenses, timeline and many others.
Furthermore, the template allows you to set different plans for online and in-store sales, making the template a must-have for your overall sales plan.
Learn more about how Visme can help you close more sales and take your business to the next level.

Create Your Action Plan Using Visme
Are you ready to create an effective action plan and track your progress while executing and running projects? Choose your favorite action plan template from the list above and start editing it using Visme’s professional document creator .
Almost every part of these templates is editable and the easy-to-use drag and drop tool helps you create action plans in a few clicks.
Sign-up for a free account in Visme today and your action plans are just a few clicks away.
Design an effective action plan quickly and easily using Visme.

Trusted by leading brands
Recommended content for you:

Create Stunning Content!
Design visual brand experiences for your business whether you are a seasoned designer or a total novice.
About the Author
Raja Antony Mandal is a Content Writer at Visme. He can quickly adapt to different writing styles, possess strong research skills, and know SEO fundamentals. Raja wants to share valuable information with his audience by telling captivating stories in his articles. He wants to travel and party a lot on the weekends, but his guitar, drum set, and volleyball court don’t let him.

Top Link Bar
- Home Currently selected
Latest On The Conservation Gateway
Conservation planning.
--> Case Studies and Plan Examples

The guidance supporting Conservation Action Planning provides you generic how-to information to guide you through the process of completing and iterating a conservation plan. However, that is not the whole story. Here you will find detailed stories about how a team tackled a step or steps in the process for their project.
To view all CAP related case studies, in the Find Resources box to the left, choose Case Study from the Resource Type drop-down menu and click Submit.
Key Resources

Latest Articles
Recently added.

Measures Brownbag Presentation: George Schuler on ENY Chapter and Caribbean Challenge

Ranking Conservation Areas in Michigan: Step-by-Step Process

Virgin Islands National Park Business Plan
Announcements, about the gateway, additional resources.
- CoolGreenScience
- Conservation Training

The Nature Conservancy is the leading conservation organization working around the world to protect ecologically important lands and waters for nature and people. VISIT NATURE.ORG»
Sign up for our free newsletter and get more of Development Asia delivered to your inbox.
Developing an Action Plan for Sustainable Consumption and Production in the Philippines

Consultations with stakeholders helped create a well-rounded sustainable and consumption action plan with broad support.
Goal 12 of the Sustainable Development Goals (SDGs)—ensure sustainable consumption and production patterns—covers a wide range of topics that could facilitate the decoupling of economic growth from natural resource use. Complementary to the concept of sustainable consumption and production (SCP) is that of the circular economy (CE)—requiring the redirection of energy and material flows from a linear to a circular direction, the transformation of waste into productive inputs, and a reduction in pollution and greenhouse gas emissions.
In 2018, supported by an Asian Development Bank technical assistance , the National Economic and Development Authority (NEDA) of the Philippines started formulating an action plan for sustainable consumption and production that supports the country's long-term vision of AmBisyon Natin 2040 —for the average Filipino to have a strongly-rooted , comfortable, secure and peaceful life by 2040. Realizing this vision requires a healthy environment and the sustainable use of natural resources to be achieved whilst pursuing continuous economic progress. However, in talking about a sustainable future for Filipinos, many are still not clear what this looks like and what needs to be done, not only at an institutional level, but also at a community and individual level.
The resulting action plan is the product of a year of research and consultation that helped achieve the following:
1. Understand the issues related to consumption and production in the Philippines, and the applicability of a circular economy model;
2. Identify pathways for intervention, and draft the action plan; and
3. Consult with stakeholders in order to refine the action plan and facilitate its adoption.
Figure 1: Methodology for Development of the Action Plan on Sustainable Consumption and Production Plan

Source: National Economic and Development Authority. 2020. Inputs to the Philippine Action Plan for Sustainable Consumption and Production (PAP4SCP) – Consultant’s Report. Mandaluyong City.
The scoping study which informed the action plan identified that the Philippines faces five key challenges in relation to achieving sustainable consumption and production:
- Continued economic, population, and urban growth, resulting in increasing demand for and pressure on natural resources in terms of stocks and pollution.
- The exponential rise in waste generated by the country in the absence of effective solid and hazardous waste management systems, meaning the waste assimilation capacity of the environment has been pushed to the limit.
- Weak enforcement of environment-related laws and regulations, and policy gaps.
- Lack of data and an effective monitoring system to evaluate the impacts of policies and programs on the environment and natural resource use.
Decisions being made now are locking in resource-intensive consumption and production patterns for generations. The United Nation’s 2030 Agenda for Sustainable Development calls for fundamental changes in the way countries produce and consume goods and services in order to minimize the impact of economic progress on the environment.
An Asian Development Bank stocktake of national responses to the environmental dimensions of the SDGs in Asia and the Pacific, including consideration of SDG 12, notes that this is a complex goal with environmental, social, and economic targets. Achieving it will require collaboration between sectors, such as energy, water, industry, and urban development. The stocktake suggests the need for ministries of finance, economy, planning and industry to share responsibility for SDG 12 with environment ministries or agencies to achieve the necessary integration.
The Philippines is one of the countries in the region developing an appropriate institutional response to SDG 12 through the formulation of an action plan for sustainable consumption and production. The Philippine Development Plan 2017-2022 has sections that address environmental issues. However, the need for an integrated approach where these environmental issues are considered by different sectors alongside the need to address other development objectives remains to be addressed. Following a sustainable consumption and production approach to economic progress should reduce the threats to the state of the environment and natural resources in the Philippines in the long-term.
Figure 2: Aspects of SDG 12

It was envisioned by NEDA that the outcome of changes in the behavior of consumers and producers would result from the adoption of a sustainable consumption and production action plan, as captured in two sub-outcomes, namely: valuing the economic, social, and environmental impacts of production and consumption processes; and enhancing the efficient and equitable resource use of firms, households, and individuals.
The first sub-outcome has two intermediate outcomes: institutionalizing natural capital accounting, and determining ecological limits and negative externalities. It refers to the need for the internalization of the economic, social, and environmental costs and benefits from consumption and production processes, in order to accurately reflect the value of impacts—both costs and benefits—of economic activities on society and the environment. The environmental and social impacts of economic processes must be assessed, and the value of natural capital and ecosystem services recognized and accounted for in order to successfully reach this sub-outcome.
The second sub-outcome has two intermediate outcomes: increased innovation and investment in green technologies and systems, and the establishment of sustainable resource allocation and equitable sharing schemes. Its intent is to initiate and enhance current efforts to promote the efficient and equitable use of resources by different stakeholders, especially firms, households, and individuals. Renewable resources must be utilized within ecological capacities and with negative externalities from extraction minimized; and innovation and investments in green technologies and facilities, and business operations/systems must be increased in order to reach this sub-outcome.
Informed by the findings of a scoping study and a review of applicability of the circular economy model to the Philippines, NEDA identified pathways for intervention under four action types:
- Promotion of sustainable consumption and production;
- Research, technology, and innovation;
- Infrastructure and the installation of green infrastructure standards, and enhancement of speed of mobility; and
- Policy creation and implementation of reforms.
Actions and activities required to achieve sustainable consumption and production were then identified, and organized into the following thematic areas:
- Resource conservation, efficiency, and cleaner production,
- Waste management, and
- Sustainable business and lifestyle.
The actions and activities were further categorized in terms of time frame (short-term, medium-term, and long-term) for planning and budgeting purposes.
Figure 3. Sustainable Consumption and Production Action Plan

The action plan for sustainable consumption and production has received broad support from other national agencies, local governments, private sector, academe, and civil society organizations. Through consultations with stakeholders, the formulation of the action plan has heightened awareness of environmental issues in the Philippines, and galvanized sectoral support for the immediate integration of the action plan into the country’s development plan.
The decision of NEDA to use a participatory approach to formulate the action plan increased awareness, reduced potential objections, and enhanced buy-in from stakeholders. Local governments were involved as NEDA realized early on the need to "localize" the action plan, requiring both horizontal and vertical policy coherence. In addition, it was important to include the private sector.
The creation of an inter-staff group within NEDA to spearhead the consultations and to facilitate the process of refining draft actions and activities enriched the action plan because it benefitted from the perspectives of different sectors. The Philippine Council for Sustainable Development (PCSD) was also reinstated and convened several times to provide overall guidance on, approval and endorsement of the action plan. It had been inactive for a long time, following its establishment to oversee the formulation of the Philippine Agenda 21 immediately after the 1992 Earth Summit, and formulation of the action plan provided a meaningful reason for its reinstatement.
ADB. 2019. Strengthening the Environmental Dimensions of the Sustainable Development Goals in Asia and the Pacific: Stocktake of National Responses to Sustainable Development Goals 12, 14 and 15. Manila: ADB.
ADB and the United Nations Environment Programme. 2019 . Strengthening the Environmental Dimensions of the Sustainable Development Goals in Asia and the Pacific: Tool Compendium . Manila: ADB.
Cruz, G. R. 2017. The Cultural Heritage-Oriented Approach to Economic Development in the Philippines: A Comparative Study of Vigan, Ilocos Sur and Escolta, Manila . Presented at the 10th De La Salle University Arts Congress, Manila.
National Economic and Development Authority. 2017. Philippine Development Plan 2017-2020 . Mandaluyong City: National Economic and Development Authority.
National Economic and Development Authority. 2020. Inputs to the Philippine Action Plan for Sustainable Consumption and Production (PAP4SCP) – Consultant’s Report. Mandaluyong City: National Economic and Development Authority.
United Nations Environment Programme. 2015. Indicators for a Resource Efficient and Green Asia and the Pacific–Measuring Progress of Sustainable Consumption and Production, Green Economy and Resource Efficiency Policies in the Asia-Pacific Region . Bangkok: United Nations Environment Programme.
United Nations Environment Programme. 2015. Sustainable Consumption and Production Global Edition, A Handbook for Policy Makers . Bangkok: United Nations Environment Programme .
Ask the Experts

Emma Marsden has over 20 years experience in the fields of environmental and sustainability assessment. Her current responsibilities include undertaking environmental safeguard compliance reviews for ADB projects, and managing preparation of the ADB Sustainability Report. Prior to ADB she worked in environmental consultancy, where she managed and coordinated environmental impact assessments, strategic environmental assessments and sustainability appraisals of policies, plans, and projects in the energy, water and urban sectors.

Agustin L. Arcenas obtained his PhD in Agricultural Economics from Michigan State University. He has worked for the World Bank and the World Food Programme. He is currently a professor at the University of the Philippines in Diliman. He has worked on and has written about various environmental and natural resource issues.

Amelia Dulce D. Supetran is an environmental management expert with more than 35 years of experience. She worked in various capacities for the Philippines’ Department of Environment and retired from the United Nations Development Programme after 15 years as team leader. She is currently a Senior Technical Adviser of the Climate Change Commission of the Philippines.

Lisa C. Antonio was executive director of the Philippine Business for the Environment. She also served as director and senior fellow of the Resource Center for Environment and Sustainable Development at the Development Academy of the Philippines, and as faculty of the Ateneo de Manila University Graduate Program on Environmental Management.

Jon Alan Cuyno has more than a decade of experience with Geocycle, the waste management unit of Holcim Philippines, Inc. He has led Geocycle teams handling pre-processing, logistics, strategy development, project and technical management. He holds a Chemical Engineering degree from the University of the Philippines in Los Baños.
The Asian Development Bank is committed to achieving a prosperous, inclusive, resilient, and sustainable Asia and the Pacific, while sustaining its efforts to eradicate extreme poverty. Established in 1966, it is owned by 68 members—49 from the region. Its main instruments for helping its developing member countries are policy dialogue, loans, equity investments, guarantees, grants, and technical assistance.
View the discussion thread.
You Might Also Like

Developing a Tool to Integrate Environmental Goals into National Sector Policies and Plans

Taking Stock of Asia's Response to Environmental Sustainability

Improving SDG Implementation in Viet Nam
The views expressed on this website are those of the authors and do not necessarily reflect the views and policies of the Asian Development Bank (ADB) or its Board of Governors or the governments they represent. ADB does not guarantee the accuracy of the data included in this publication and accepts no responsibility for any consequence of their use. By making any designation of or reference to a particular territory or geographic area, or by using the term “country” in this document, ADB does not intend to make any judgments as to the legal or other status of any territory or area.
- Agriculture and natural resources
- Capacity development
- Civil society
- Climate change
- Environment
- Finance sector development
- Governance and public sector management
- Industry and trade
- Information and communications technology
- Private sector development
- Regional cooperation and integration
- Social development and protection
- Urban development
- Afghanistan
- China, People's Republic of
- Cook Islands
- Korea, Republic of
- Kyrgyz Republic
- Lao People's Democratic Republic
- Marshall Islands
- New Zealand
- Papua New Guinea
- Philippines
- Solomon Islands
- Timor-Leste
- Turkmenistan
- Goal 1: No Poverty
- Goal 2: Zero Hunger
- Goal 3: Good Health and Well-being
- Goal 4: Quality Education
- Goal 5: Gender Equality
- Goal 6: Clean Water and Sanitation
- Goal 7: Affordable and Clean Energy
- Goal 8: Decent Work and Economic Growth
- Goal 9: Industry, Innovation and Infrastructure
- Goal 10: Reduced Inequalities
- Goal 11: Sustainable Cities and Communities
- Goal 12: Responsible Consumption and Production
- Goal 13: Climate Action
- Goal 14: Life Below Water
- Goal 15: Life on Land
- Goal 16: Peace, Justice and Strong Institutions
- Goal 17: Partnerships for the Goals
- All Content
- Communities
Pardon Our Interruption
As you were browsing something about your browser made us think you were a bot. There are a few reasons this might happen:
- You've disabled JavaScript in your web browser.
- You're a power user moving through this website with super-human speed.
- You've disabled cookies in your web browser.
- A third-party browser plugin, such as Ghostery or NoScript, is preventing JavaScript from running. Additional information is available in this support article .
To regain access, please make sure that cookies and JavaScript are enabled before reloading the page.
Home » Education » Difference Between Action Research and Case Study
Difference Between Action Research and Case Study
Main difference – action research vs case study.
Research is the careful study of a given field or problem in order to discover new facts or principles. Action research and case study are two types of research, which are mainly used in the field of social sciences and humanities. The main difference between action research and case study is their purpose; an action research study aims to solve an immediate problem whereas a case study aims to provide an in-depth analysis of a situation or case over a long period of time.
1. What is Action Research? – Definition, Features, Purpose, Process
2. What is Case Study? – Definition, Features, Purpose, Process

What is Action Research
Action research is a type of a research study that is initiated to solve an immediate problem. It may involve a variety of analytical, investigative and evaluative research methods designed to diagnose and solve problems. It has been defined as “a disciplined process of inquiry conducted by and for those taking the action. The primary reason for engaging in action research is to assist the “actor” in improving and/or refining his or her actions” (Sagor, 2000). This type of research is typically used in the field of education. Action research studies are generally conductors by educators, who also act as participants.
Here, an individual researcher or a group of researchers identify a problem, examine its causes and try to arrive at a solution to the problem. The action research process is as follows.
Action Research Process
- Identify a problem to research
- Clarify theories
- Identify research questions
- Collect data on the problem
- Organise, analyse, and interpret the data
- Create a plan to address the problem
- Implement the above-mentioned plan
- Evaluate the results of the actions taken
The above process will keep repeating. Action research is also known as cycle of inquiry or cycle of action since it follows a specific process that is repeated over time.

What is a Case Study
A case study is basically an in-depth examination of a particular event, situation or an individual. It is a type of research that is designed to explore and understand complex issues; however, it involves detailed contextual analysis of only a limited number of events or situations. It has been defined as “an empirical inquiry that investigates a contemporary phenomenon within its real-life context; when the boundaries between phenomenon and context are not clearly evident; and in which multiple sources of evidence are used.” (Yin, 1984)
Case studies are used in a variety of fields, but fields like sociology and education seem to use them the most. They can be used to probe into community-based problems such as illiteracy, unemployment, poverty, and drug addiction.
Case studies involve both quantitative and qualitative data and allow the researchers to see beyond statistical results and understand human conditions. Furthermore, case studies can be classified into three categories, known as exploratory, descriptive and explanatory case studies.
However, case studies are also criticised since the study of a limited number of events or cases cannot easily establish generality or reliability of the findings. The process of a case study is generally as follows:
Case Study Process
- Identifying and defining the research questions
- Selecting the cases and deciding techniques for data collection and analysis
- Collecting data in the field
- Evaluating and analysing the data
- Preparing the report
Action Research : Action research is a type of a research study that is initiated to solve an immediate problem.
Case Study : Case study is an in-depth analysis of a particular event or case over a long period of time.
Action Research : Action research involves solving a problem.
Case Study : Case studies involve observing and analysing a situation.
Action Research : Action research studies are mainly used in the field of education.
Case Study : Case studies are used in many fields; they can be specially used with community problems such as unemployment, poverty, etc.
Action Research : Action research always involve providing a solution to a problem.
Case Study : Case studies do not provide a solution to a problem.
Participants
Action Research : Researchers can also act as participants of the research.
Case Study : Researchers generally don’t take part in the research study.
Zainal, Zaidah. Case study as a research method . N.p.: n.p., 7 June 2007. PDF.
Soy, Susan K. (1997). The case study as a research method . Unpublished paper, University of Texas at Austin.
Sagor, Richard. Guiding school improvement with action research . Ascd, 2000.
Image Courtesy: Pixabay

About the Author: Hasa
Hasanthi is a seasoned content writer and editor with over 8 years of experience. Armed with a BA degree in English and a knack for digital marketing, she explores her passions for literature, history, culture, and food through her engaging and informative writing.
You May Also Like These
Leave a reply cancel reply.
- Open access
- Published: 10 August 2024
How can health systems approach reducing health inequalities? An in-depth qualitative case study in the UK
- Charlotte Parbery-Clark 1 ,
- Lorraine McSweeney 2 ,
- Joanne Lally 3 &
- Sarah Sowden 4
BMC Public Health volume 24 , Article number: 2168 ( 2024 ) Cite this article
314 Accesses
Metrics details
Addressing socioeconomic inequalities in health and healthcare, and reducing avoidable hospital admissions requires integrated strategy and complex intervention across health systems. However, the understanding of how to create effective systems to reduce socio-economic inequalities in health and healthcare is limited. The aim was to explore and develop a system’s level understanding of how local areas address health inequalities with a focus on avoidable emergency admissions.
In-depth case study using qualitative investigation (documentary analysis and key informant interviews) in an urban UK local authority. Interviewees were identified using snowball sampling. Documents were retrieved via key informants and web searches of relevant organisations. Interviews and documents were analysed independently based on a thematic analysis approach.
Interviews ( n = 14) with wide representation from local authority ( n = 8), NHS ( n = 5) and voluntary, community and social enterprise (VCSE) sector ( n = 1) with 75 documents (including from NHS, local authority, VCSE) were included. Cross-referenced themes were understanding the local context, facilitators of how to tackle health inequalities: the assets, and emerging risks and concerns. Addressing health inequalities in avoidable admissions per se was not often explicitly linked by either the interviews or documents and is not yet embedded into practice. However, a strong coherent strategic integrated population health management plan with a system’s approach to reducing health inequalities was evident as was collective action and involving people, with links to a “strong third sector”. Challenges reported include structural barriers and threats, the analysis and accessibility of data as well as ongoing pressures on the health and care system.
We provide an in-depth exploration of how a local area is working to address health and care inequalities. Key elements of this system’s working include fostering strategic coherence, cross-agency working, and community-asset based approaches. Areas requiring action included data sharing challenges across organisations and analytical capacity to assist endeavours to reduce health and care inequalities. Other areas were around the resilience of the system including the recruitment and retention of the workforce. More action is required to embed reducing health inequalities in avoidable admissions explicitly in local areas with inaction risking widening the health gap.
Highlights:
• Reducing health inequalities in avoidable hospital admissions is yet to be explicitly linked in practice and is an important area to address.
• Understanding the local context helps to identify existing assets and threats including the leverage points for action.
• Requiring action includes building the resilience of our complex systems by addressing structural barriers and threats as well as supporting the workforce (training and wellbeing with improved retention and recruitment) in addition to the analysis and accessibility of data across the system.
Peer Review reports
Introduction
The health of our population is determined by the complex interaction of several factors which are either non-modifiable (such as age, genetics) or modifiable (such as the environment, social, economic conditions in which we live, our behaviours as well as our access to healthcare and its quality) [ 1 ]. Health inequalities are the avoidable and unfair systematic differences in health and healthcare across different population groups explained by the differences in distribution of power, wealth and resources which drive the conditions of daily life [ 2 , 3 ]. Essentially, health inequalities arise due to the systematic differences of the factors that influence our health. To effectively deal with most public health challenges, including reducing health inequalities and improving population health, broader integrated approaches [ 4 ] and an emphasis on systems is required [ 5 , 6 ] . A system is defined as ‘the set of actors, activities, and settings that are directly or indirectly perceived to have influence in or be affected by a given problem situation’ (p.198) [ 7 ]. In this case, the ‘given problem situation' is reducing health inequalities with a focus on avoidable admissions. Therefore, we must consider health systems, which are the organisations, resources and people aiming to improve or maintain health [ 8 , 9 ] of which health services provision is an aspect. In this study, the system considers NHS bodies, Integrated Care Systems, Local Authority departments, and the voluntary and community sector in a UK region.
A plethora of theories [ 10 ], recommended policies [ 3 , 11 , 12 , 13 ], frameworks [ 1 , 14 , 15 ], and tools [ 16 ] exist to help understand the existence of health inequalities as well as provide suggestions for improvement. However, it is reported that healthcare leaders feel under-skilled to reduce health inequalities [ 17 ]. A lack of clarity exists on how to achieve a system’s multi-agency coherence to reduce health inequalities systematically [ 17 , 18 ]. This is despite some countries having legal obligations to have a regard to the need to attend to health and healthcare inequalities. For example, the Health and Social Care Act 2012 [ 19 ], in England, mandated Clinical Commissioning Groups (CCGs), now transferred to Integrated Care Boards (ICBs) [ 20 ], to ‘have a regard to the need to reduce inequalities between patients with respect to their ability to access health services, and reduce inequalities between patients with respect to the outcomes achieved for them by the provision of health services’. The wider determinants of health must also be considered. For example, local areas have a mandatory requirement to have a joint strategic needs assessment (JSNA) and joint health and wellbeing strategy (JHWS) whose purpose is to ‘improve the health and wellbeing of the local community and reduce inequalities for all ages' [ 21 ] This includes addressing the wider determinants of health [ 21 ]. Furthermore, the hospital care costs to the NHS associated with socioeconomic inequalities has been previously reported at £4.8 billion a year due to excess hospitalisations [ 22 ]. Avoidable emergency admissions are admissions into hospital that are considered to be preventable with high-quality ambulatory care [ 23 ]. Both ambulatory care sensitive conditions (where effective personalised care based in the community can aid the prevention of needing an admission) and urgent care sensitive conditions (where a system on the whole should be able to treat and manage without an admission) are considered within this definition [ 24 ] (encompassing more than 100 International Classification of Diseases (ICD) codes). The disease burden sits disproportionately with our most disadvantaged communities, therefore highlighting the importance of addressing inequalities in hospital pressures in a concerted manner [ 25 , 26 ].
Research examining one component of an intervention, or even one part of the system, [ 27 ] or which uses specific research techniques to control for the system’s context [ 28 ] are considered as having limited use for identifying the key ingredients to achieve better population health and wellbeing [ 5 , 28 ]. Instead, systems thinking considers how the system’s components and sub-components interconnect and interrelate within and between each other (and indeed other systems) to gain an understanding of the mechanisms by which things work [ 29 , 30 ]. Complex interventions or work programmes may perform differently in varying contexts and through different mechanisms, and therefore cannot simply be replicated from one context to another to automatically achieve the same outcomes. Ensuring that research into systems and systems thinking considers real-world context, such as where individuals live, where policies are created and interventions are delivered, is vital [ 5 ]. How the context and implementation of complex or even simple interventions interact is viewed as becoming increasingly important [ 31 , 32 ]. Case study research methodology is founded on the ‘in-depth exploration of complex phenomena in their natural, or ‘real-life’, settings’ (p.2) [ 33 ]. Case study approaches can deepen the understanding of complexity addressing the ‘how’, ‘what’ and ‘why’ questions in a real-life context [ 34 ]. Researchers have highlighted the importance of engaging more deeply with case-based study methodology [ 31 , 33 ]. Previous case study research has shown promise [ 35 ] which we build on by exploring a systems lens to consider the local area’s context [ 16 ] within which the work is implemented. By using case-study methodology, our study aimed to explore and develop an in-depth understanding of how a local area addresses health inequalities, with a focus on avoidable hospital admissions. As part of this, systems processes were included.
Study design
This in-depth case study is part of an ongoing larger multiple (collective [ 36 ]) case study approach. An instrumental approach [ 34 ] was taken allowing an in-depth investigation of an issue, event or phenomenon, in its natural real-life context; referred to as a ‘naturalistic’ design [ 34 ]. Ethics approval was obtained by Newcastle University’s Ethics Committee (ref 13633/2020).
Study selection
This case study, alongside the other three cases, was purposively [ 36 ] chosen considering overall deprivation level of the area (Indices of Multiple Deprivation (IMD) [ 37 ]), their urban/rural location, differing geographical spread across the UK (highlighted in patient and public feedback and important for considering the North/South health divide [ 38 ]), and a pragmatic judgement of likely ability to achieve the depth of insight required [ 39 ]. In this paper, we report the findings from one of the case studies, an urban local authority in the Northern region of the UK with high levels of socioeconomic disadvantage. This area was chosen for this in-depth case analysis due to high-level of need, and prior to the COVID-19 pandemic (2009-2018) had experienced a trend towards reducing socioeconomic inequalities in avoidable hospital admission rates between neighbourhoods within the local area [ 40 ]. Thereby this case study represents an ‘unusual’ case [ 41 ] to facilitate learning regarding what is reported and considered to be the key elements required to reduce health inequalities, including inequalities in avoidable admissions, in a local area.
Semi-structured interviews
The key informants were identified iteratively through the documentary analysis and in consultation with the research advisory group. Initially board level committee members (including lay, managerial, and clinical members) within relevant local organisations were purposively identified. These individuals were systems leaders charged with the remit of tackling health inequalities and therefore well placed to identify both key personnel and documents. Snowball sampling [ 42 ] was undertaken thereafter whereby interviewees helped to identify additional key informants within the local system who were working on health inequalities, including avoidable emergency admissions, at a systems level. Interview questions were based on an iteratively developed topic guide (supplementary data 1), informed from previous work’s findings [ 43 ] and the research advisory network’s input. A study information sheet was emailed to perspective interviewees, and participants were asked to complete an e-consent form using Microsoft Forms [ 42 ]. Each interviewee was interviewed by either L.M. or C.P.-C. using the online platforms Zoom or Teams, and lasted up to one hour. Participants were informed of interviewers’ role, workplace as well as purpose of the study. Interviewees were asked a range of questions including any work relating to reducing health inequalities, particularly avoidable emergency admissions, within the last 5 years. Brief notes were taken, and the interviews were recorded, transcribed verbatim and anonymised.
Documentary analysis
The documentary analysis followed the READ approach [ 44 ]. Any documents from the relevant local/regional area with sections addressing health inequalities and/or avoidable emergency admissions, either explicitly stated or implicitly inferred, were included. A list of core documents was chosen, including the local Health and Wellbeing Strategy (Table 1 ). Subsequently, other documents were identified by snowballing from these core documents and identification by the interviewees. All document types were within scope if produced/covered a period within 5 years (2017-2022), including documents in the public domain or not as well as documents pertaining to either a regional, local and neighbourhood level. This 5-year period was a pragmatic decision in line with the interviews and considered to be a balance of legacy and relevance. Attempts were made to include the final version of each document, where possible/applicable, otherwise the most up-to-date version or version available was used.
An Excel spreadsheet data extraction tool was adapted with a priori criteria [ 44 ] to extract the data. This tool included contextual information (such as authors, target area and document’s purpose). Also, information based on previous research on addressing socioeconomic inequalities in avoidable emergency admissions, such as who stands to benefit, was extracted [ 43 ]. Additionally, all documents were summarised according to a template designed according to the research’s aims. Data extraction and summaries were undertaken by L.M. and C.P.-C. A selection was doubled coded to enhance validity and any discrepancies were resolved by discussion.
Interviews and documents were coded and analysed independently based on a thematic analysis approach [ 45 ], managed by NVivo software. A combination of ‘interpretive’ and ‘positivist’ stance [ 34 , 46 ] was taken which involved understanding meanings/contexts and processes as perceived from different perspectives (interviewees and documents). This allowed for an understanding of individual and shared social meanings/reasonings [ 34 , 36 ]. For the documentary analysis, a combination of both content and thematic analysis as described by Bowen [ 47 ] informed by Braun and Clarke’s approach to thematic analysis [ 45 ] was used. This type of content analysis does not include the typical quantification but rather a review of the document for pertinent and meaningful passages of text/other data [ 47 ]. Both an inductive and deductive approach for the documentary analysis’ coding [ 46 , 47 ] was chosen. The inductive approach was developed a posteriori; the deductive codes being informed by the interviews and previous findings from research addressing socioeconomic inequalities in avoidable emergency admissions [ 43 ]. In line with qualitative epistemological approach to enquiry, the interview and documentary findings were viewed as ‘truths’ in themselves with the acceptance that multiple realities can co-exist [ 48 ]. The analysis of each set of themes (with subthemes) from the documentary analysis and interviews were cross-referenced and integrated with each other to provide a cohesive in-depth analysis [ 49 ] by generating thematic maps to explore the relationships between the themes. The codes, themes and thematic maps were peer-reviewed continually with regular meetings between L.M., C.P.-C., J.L. and S.S. Direct quotes are provided from the interviews and documentary analysis. Some quotes from the documents are paraphrased to protect anonymity of the case study after following a set process considering a range of options. This involved searching each quote from the documentary analysis in Google and if the quote was found in the first page of the result, we shortened extracts and repeated the process. Where the shortened extracts were still identifiable, we were required to paraphrase that quote. Each paraphrased quote and original was shared and agreed with all the authors reducing the likelihood of inadvertently misinterpreting or misquoting. Where multiple components over large bodies of text were present in the documents, models were used to evidence the broadness, for example, using Dahlgren’s and Whitehead’s model of health determinants [ 1 ]. Due to the nature of the study, transcripts and findings were not shared with participants for checking but will be shared in a dissemination workshop in 2024.
Patient and public involvement and engagement
Four public contributors from the National Institute for Health and Care Research (NIHR) Research Design Service (RDS) North East and North Cumbria (NENC) Public and Patient Involvement (PPI) panel have been actively engaged in this research from its inception. They have been part of the research advisory group along with professional stakeholders and were involved in the identification of the sampling frame’s key criteria. Furthermore, a diverse group of public contributors has been actively involved in other parts of the project including developing the moral argument around action by producing a public facing resource exploring what health inequalities mean to people and public views of possible solutions [ 50 ].
Semi-structured interviews: description
Sixteen participants working in health or social care, identified through the documentary analysis or snowballing, were contacted for interview; fourteen consented to participate. No further interviews were sought as data sufficiency was reached whereby no new information or themes were being identified. Participant roles were broken down by NHS ( n = 5), local authority/council ( n = 8), and voluntary, community and social enterprise (VSCE) ( n = 1). To protect the participants’ anonymity, their employment titles/status are not disclosed. However, a broad spectrum of interviewees with varying roles from senior health system leadership (including strategic and commissioner roles) to roles within provider organisations and the VSCE sector were included.
Documentary analysis: description
75 documents were reviewed with documents considering regional ( n = 20), local ( n = 64) or neighbourhood ( n = 2) area with some documents covering two or more areas. Table 2 summarises the respective number of each document type which included statutory documents to websites from across the system (NHS, local government and VSCE). 45 documents were named by interviewees and 42 documents were identified as either a core document or through snowballing from other documents. Of these, 12 documents were identified from both. The timescales of the documents varied and where possible to identify, was from 2014 to 2031.
Integrative analysis of the documentary analysis and interviews
The overarching themes encompass:
Understanding the local context
Facilitators to tacking health inequalities: the assets
Emerging risks and concerns
Figure 1 demonstrates the relationships between the main themes identified from the analysis for tackling health inequalities and improving health in this case study.

Diagram of the relationship between the key themes identified regarding tackling health inequalities and improving health in a local area informed by 2 previous work [ 14 , 51 ]. NCDs = non-communicable diseases; HI = health inequalities
Understanding the local context was discussed extensively in both the documents and the interviews. This was informed by local intelligence and data that was routinely collected, monitored, and analysed to help understand the local context and where inequalities lie. More bespoke, in-depth collection and analysis were also described to get a better understanding of the situation. This not only took the form of quantitative but also considered qualitative data with lived experience:
‛So, our data comes from going out to talk to people. I mean, yes, especially the voice of inequalities, those traditional mechanisms, like surveys, don't really work. And it's about going out to communities, linking in with third sector organisations, going out to communities, and just going out to listen…I think the more we can bring out those real stories. I mean, we find quotes really, really powerful in terms of helping people understand what it is that matters.’ (LP16).
However, there were limitations to the available data including the quality as well as having enough time to do the analysis justice. This resulted in difficulties in being able to fully understand the context to help identify and act on the required improvements.
‘A lack of available data means we cannot quantify the total number of vulnerable migrants in [region]’ (Document V).
‛So there’s lots of data. The issue is joining that data up and analysing it, and making sense of it. That’s where we don’t have the capacity.’ (LP15).
Despite the caveats, understanding the context and its data limitations were important to inform local priorities and approaches on tackling health inequalities. This understanding was underpinned by three subthemes which were understanding:
the population’s needs including identification of people at higher risk of worse health and health inequalities
the driving forces of those needs with acknowledgement of the impact of the wider determinants of health
the threats and barriers to physical and mental health, as well as wellbeing
Firstly, the population’s needs, including identification of people at higher risk of worse health and health inequalities, was important. This included considering risk factors, such as smoking, specific groups of people and who was presenting with which conditions. Between the interviews and documents, variation was seen between groups deemed at-risk or high-risk with the documents identifying a wider range. The groups identified across both included marginalised communities, such as ethnic minority groups, gypsy and travellers, refugees and asylum seekers as well as people/children living in disadvantaged area.
‘There are significant health inequalities in children with asthma between deprived and more affluent areas, and this is reflected in A&E admissions.' (Document J).
Secondly, the driving forces of those needs with acknowledgement of the impact of the wider determinants of health were described. These forces mapped onto Dahlgren’s and Whitehead’s model of health determinants [ 1 ] consisting of individual lifestyle factors, social and community networks, living and working conditions (which include access to health care services) as well as general socio-economic, cultural and environmental conditions across the life course.
…. at the centre of our approach considering the requirements to improve the health and wellbeing of our area are the wider determinants of health and wellbeing, acknowledging how factors, such as housing, education, the environment and economy, impact on health outcomes and wellbeing over people’s lifetime and are therefore pivotal to our ambition to ameliorate the health of the poorest the quickest. (Paraphrased Document P).
Thirdly, the threats and barriers to health included environmental risks, communicable diseases and associated challenges, non-communicable conditions and diseases, mental health as well as structural barriers. In terms of communicable diseases, COVID-19 predominated. The environmental risks included climate change and air pollution. Non-communicable diseases were considered as a substantial and increasing threat and encompassed a wide range of chronic conditions such as diabetes, and obesity.
‛Long term conditions are the leading causes of death and disability in [case study] and account for most of our health and care spending. Cases of cancer, diabetes, respiratory disease, dementia and cardiovascular disease will increase as the population of [case study] grows and ages.’ (Document A).
Structural barriers to accessing and using support and/or services for health and wellbeing were identified. These barriers included how the services are set up, such as some GP practices asking for proof of a fixed address or form of identification to register. For example:
Complicated systems (such as having to make multiple calls, the need to speak to many people/gatekeepers or to call at specific time) can be a massive barrier to accessing healthcare and appointments. This is the case particularly for people who have complex mental health needs or chaotic/destabilized circumstances. People who do not have stable housing face difficulties in registering for GP and other services that require an address or rely on post to communicate appointments. (Paraphrased Document R).
A structural threat regarding support and/or services for health and wellbeing was the sustainability of current funding with future uncertainty posing potential threats to the delivery of current services. This also affected the ability to adapt and develop the services, or indeed build new ones.
‛I would say the other thing is I have a beef [sic] [disagreement] with pilot studies or new innovations. Often soft funded, temporary funded, charity funded, partnership work run by enthusiasts. Me, I've done them, or supported people doing many of these. And they're great. They can make a huge impact on the individuals involved on that local area. You can see fantastic work. You get inspired and you want to stand up in a crowd and go, “Wahey, isn't this fantastic?” But actually the sad part of it is on these things, I've seen so many where we then see some good, positive work being done, but we can't make it permanent or we can't spread it because there's no funding behind it.’ (LP8).
Facilitators to tackling health inequalities: the assets
The facilitators for improving health and wellbeing and tackling health inequalities are considered as assets which were underpinned by values and principles.
Values driven supported by four key principles
Being values driven was an important concept and considered as the underpinning attitudes or beliefs that guide decision making [ 52 ]. Particularly, the system’s approach was underpinned by a culture and a system's commitment to tackle health inequalities across the documents and interviews. This was also demonstrated by how passionately and emotively some interviewees spoke about their work.
‛There's a really strong desire and ethos around understanding that we will only ever solve these problems as a system, not by individual organisations or even just part of the system working together. And that feels great.’ (LP3).
Other values driving the approach included accountability, justice, and equity. Reducing health inequalities and improving health were considered to be the right things to do. For example:
We feel strongly about social justice and being inclusive, wishing to reflect the diversity of [case study]. We campaign on subjects that are important to people who are older with respect and kindness. (Paraphrased Document O).
Four key principles were identified that crosscut the assets which were:
Shared vision
Strong partnership
Asset-based approaches
Willingness and ability to act on learning
The mandated strategy, identifying priorities for health and wellbeing for the local population with the required actions, provided the shared vision across each part of the system, and provided the foundations for the work. This shared vision was repeated consistently in the documents and interviews from across the system.
[Case study] will be a place where individuals who have the lowest socioeconomic status will ameliorate their health the quickest. [Case study] will be a place for good health and compassion for all people, regardless of their age. (Paraphrased Document A).
‛One thing that is obviously becoming stronger and stronger is the focus on health inequalities within all of that, and making sure that we are helping people and provide support to people with the poorest health as fast as possible, so that agenda hasn’t shifted.’ (LP7).
This drive to embed the reduction of health inequalities was supported by clear new national guidance encapsulated by the NHS Core20PLUS5 priorities. Core20PLUS5 is the UK's approach to support a system to improve their healthcare inequalities [ 53 ]. Additionally, the system's restructuring from Clinical Commissioning Groups (CCGs) to Integrated Care Boards (ICBs) and formalisation of the now statutory Integrated Care Systems (ICS) in England was also reported to facilitate the driving of further improvement in health inequalities. These changes at a regional and local level helped bring key partners across the system (NHS and local government among others) to build upon their collective responsibility for improving health and reducing health inequalities for their area [ 54 ].
‛I don’t remember the last time we’ve had that so clear, or the last time that health inequalities has had such a prominent place, both in the NHS planning guidance or in the NHS contract. ’ (LP15). ‛The Health and Care Act has now got a, kind of, pillar around health inequalities, the new establishment of ICPs and ICBs, and also the planning guidance this year had a very clear element on health inequalities.’ (LP12)
A strong partnership and collaborative team approach across the system underpinned the work from the documents and included the reoccurrence of the concept that this case study acted as one team: ‘Team [case study]'.
Supporting one another to ensure [case study] is the best it can be: Team [case study]. It involves learning, sharing ideas as well as organisations sharing assets and resources, authentic partnerships, and striving for collective impact (environmental and social) to work towards shared goals . (Paraphrased Document B).
This was corroborated in the interviews as working in partnership to tackle health inequalities was considered by the interviewees as moving in the right direction. There were reports that the relationship between local government, health care and the third sector had improved in recent years which was still an ongoing priority:
‘I think the only improvement I would cite, which is not an improvement in terms of health outcomes, but in terms of how we work across [case study] together has moved on quite a lot, in terms of teams leads and talking across us, and how we join up on things, rather than see ourselves all as separate bodies' (LP15).
‘I think the relationship between local authorities and health and the third sector, actually, has much more parity and esteem than it had before.' (LP11)
The approaches described above were supported by all health and care partners signing up to principles around partnership; it is likely this has helped foster the case study's approach. This also builds on the asset-based approaches that were another key principle building on co-production and co-creation which is described below.
We begin with people : instead of doing things to people or for them, we work with them, augmenting the skills, assets and strength of [case study]’s people, workforce and carers. We achieve : actions are focused on over words and by using intelligence, every action hones in on the actual difference that we will make to ameliorate outcomes, quality and spend [case study]’s money wisely; We are Team [case study ]: having kindness, working as one organisation, taking responsibility collectively and delivering on what we agreed. Problems are discussed with a high challenge and high support attitude. (Paraphrased Document D).
At times, the degree to which the asset-based approaches were embedded differed from the documents compared to the interviews, even when from the same part of the system. For example, the documents often referred to the asset-based approach as having occurred whilst interviewees viewed it more as a work in progress.
‘We have re-designed many of our services to focus on needs-led, asset-based early intervention and prevention, and have given citizens more control over decisions that directly affect them .’ (Document M).
‘But we’re trying to take an asset-based approach, which is looking at the good stuff in communities as well. So the buildings, the green space, the services, but then also the social capital stuff that happens under the radar.’ (LP11).
A willingness to learn and put in action plans to address the learning were present. This enables future proofing by building on what is already in place to build the capacity, capability and flexibility of the system. This was particularly important for developing the workforce as described below.
‘So we’ve got a task and finish group set up, […] So this group shows good practice and is a space for people to discuss some of the challenges or to share what interventions they are doing around the table, and also look at what other opportunities that they have within a region or that we could build upon and share and scale.’ (LP12).
These assets that are considered as facilitators are divided into four key levels which are the system, services and support, communities and individuals, and workforce which are discussed in turn below.
Firstly, the system within this case study was made up of many organisations and partnerships within the NHS, local government, VSCE sector and communities. The interviewees reported the presence of a strong VCSE sector which had been facilitated by the local council's commitment to funding this sector:
‘Within [case study], we have a brilliant third sector, the council has been longstanding funders of infrastructure in [case study], third sector infrastructure, to enable those links [of community engagement] to be made' (LP16).
In both the documents and interviews, a strong coherent strategic integrated population health management plan with a system’s approach to embed the reduction of health inequalities was evident. For example, on a system level regionally:
‘To contribute towards a reduction in health inequalities we will: take a system wide approach for improving outcomes for specific groups known to be affected by health inequalities, starting with those living in our most deprived communities….’ (Document H).
This case study’s approach within the system included using creative solutions and harnessing technology. This included making bold and inventive changes to improve how the city and the system linked up and worked together to improve health. For example, regeneration work within the city to ameliorate and transform healthcare facilities as well as certain neighbourhoods by having new green spaces, better transport links in order to improve city-wide innovation and collaboration (paraphrased Document F) were described. The changes were not only related to physical aspects of the city but also aimed at how the city digitally linked up. Being a leader in digital innovation to optimise the health benefits from technology and information was identified in several documents.
‘ Having the best connected city using digital technology to improve health and wellbeing in innovative ways.’ (Document G).
The digital approaches included ongoing development of a digitalised personalised care record facilitating access to the most up-to-date information to developing as well as having the ‘ latest, cutting edge technologies’ ( Document F) in hospital care. However, the importance of not leaving people behind by embedding digital alternatives was recognised in both the documents and interviews.
‘ We are trying to just embed the culture of doing an equity health impact assessment whenever you are bringing in a digital solution or a digital pathway, and that there is always an alternative there for people who don’t have the capability or capacity to use it. ’ (LP1).
The successful one hundred percent [redacted] programme is targeting some of our most digitally excluded citizens in [case study]. For our city to continue to thrive, we all need the appropriate skills, technology and support to get the most out of being online. (Paraphrased Document Q)
This all links in with the system that functions in a ‘place' which includes the importance of where people are born, grow, work and live. Working towards this place being welcoming and appealing was described both regionally and locally. This included aiming to make the case study the place of choice for people.
‘Making [case study] a centre for good growth becoming the place of choice in the UK to live, to study, for businesses to invest in, for people to come and work.’ (Document G).
Services and support
Secondly, a variety of available services and support were described from the local authority, NHS, and voluntary community sectors. Specific areas of work, such as local initiatives (including targeted work or campaigns for specific groups or specific health conditions) as well as parts of the system working together with communities collaboratively, were identified. This included a wide range of work being done such as avoiding delayed discharges or re-admissions, providing high quality affordable housing as well as services offering peer support.
‘We have a community health development programme called [redacted], that works with particular groups in deprived communities and ethnically diverse communities to work in a very trusted and culturally appropriate way on the things that they want to get involved with to support their health.’ (LP3 ).
It is worth noting that reducing health inequalities in avoidable admissions was not often explicitly specified in the documents or interviews. However, either specified or otherwise inferred, preventing ill health and improving access, experience, and outcomes were vital components to addressing inequalities. This was approached by working with communities to deliver services in communities that worked for all people. Having co-designed, accessible, equitable integrated services and support appeared to be key.
‘Reducing inequalities in unplanned admissions for conditions that could be cared for in the community and access to planned hospital care is key.’ (Document H)
Creating plans with people: understanding the needs of local population and designing joined-up services around these needs. (Paraphrased Document A).
‘ So I think a core element is engagement with your population, so that ownership and that co-production, if you're going to make an intervention, don't do it without because you might miss the mark. ’ (LP8).
Clear, consistent and appropriate communication that was trusted was considered important to improve health and wellbeing as well as to tackle health inequalities. For example, trusted community members being engaged to speak on the behalf of the service providers:
‘The messenger is more important than the message, sometimes.’ (LP11).
This included making sure the processes are in place so that the information is accessible for all, including people who have additional communication needs. This was considered as a work in progress in this case study.
‘I think for me, things do come down to those core things, of health, literacy, that digital exclusion and understanding the wider complexities of people.’ (LP12)
‘ But even more confusing if you've got an additional communication need. And we've done quite a lot of work around the accessible information standard which sounds quite dry, and doesn't sound very- but actually, it's fundamental in accessing health and care. And that is, that all health and care organisations should record your communication preferences. So, if I've got a learning disability, people should know. If I've got a hearing impairment, people should know. But the systems don’t record it, so blind people are getting sent letters for appointments, or if I've got hearing loss, the right provisions are not made for appointments. So, actually, we're putting up barriers before people even come in, or can even get access to services.’ (LP16).
Flexible, empowering, holistic care and support that was person-centric was more apparent in the documents than the interviews.
At the centre of our vision is having more people benefiting from the life chances currently enjoyed by the few to make [case study] a more equal place. Therefore, we accentuate the importance of good health, the requirement to boost resilience, and focus on prevention as a way of enabling higher quality service provision that is person-centred. [Paraphrased Document N).
Through this [work], we will give all children and young people in [case study], particularly if they are vulnerable and/or disadvantaged, a start in life that is empowering and enable them to flourish in a compassionate and lively city. [Paraphrased Document M].
Communities and individuals
Thirdly, having communities and individuals at the heart of the work appeared essential and viewed as crucial to nurture in this case study. The interconnectedness of the place, communities and individuals were considered a key part of the foundations for good health and wellbeing.
In [case study], our belief is that our people are our greatest strength and our most important asset. Wellbeing starts with people: our connections with our friends, family, and colleagues, our behaviour, understanding, and support for one another, as well as the environment we build to live in together . (Paraphrased Document A).
A recognition of the power of communities and individuals with the requirement to support that key principle of a strength-based approach was found. This involved close working with communities to help identify what was important, what was needed and what interventions would work. This could then lead to improved resilience and cohesion.
‛You can't make effective health and care decisions without having the voice of people at the centre of that. It just won't work. You won't make the right decisions.’ (LP16).
‘Build on the strengths in ourselves, our families, carers and our community; working with people, actively listening to what matters most to people, with a focus on what’s strong rather than what’s wrong’ (Document G).
Meaningful engagement with communities as well as strengths and asset-based approaches to ensure self-sufficiency and sustainability of communities can help communities flourish. This includes promoting friendships, building community resilience and capacity, and inspiring residents to find solutions to change the things they feel needs altering in their community . (Paraphrased Document B).
This close community engagement had been reported to foster trust and to lead to improvements in health.
‘But where a system or an area has done a lot of community engagement, worked really closely with the community, gained their trust and built a programme around them rather than just said, “Here it is. You need to come and use it now,” you can tell that has had the impact. ' (LP1).
Finally, workforce was another key asset; the documents raised the concept of one workforce across health and care. The key principles of having a shared vision, asset-based approaches and strong partnership were also present in this example:
By working together, the Health and Care sector makes [case study] the best area to not only work but also train for people of all ages. Opportunities for skills and jobs are provided with recruitment and engagement from our most disadvantaged communities, galvanizing the future’s health and care workforce. By doing this, we have a very skilled and diverse workforce we need to work with our people now as well as in the future. (Paraphrased Document E).
An action identified for the health and care system to address health inequalities in case study 1 was ‘ the importance of having an inclusive workforce trained in person-centred working practices ’ (Document R). Several ways were found to improve and support workforce skills development and embed awareness of health inequalities in practice and training. Various initiatives were available such as an interactive health inequalities toolkit, theme-related fellowships, platforms and networks to share learning and develop skills.
‛We've recently launched a [redacted] Fellowship across [case study’s region], and we've got a number of clinicians and managers on that………. We've got training modules that we've put on across [case study’s region], as well for health inequalities…we've got learning and web resources where we share good practice from across the system, so that is our [redacted] Academy.’ (LP2).
This case study also recognised the importance of considering the welfare of the workforce; being skilled was not enough. This had been recognised pre-pandemic but was seen as even more important post COVID-19 due to the impact that COVID-19 had on staff, particularly in health and social care.
‛The impacts of the pandemic cannot be underestimated; our colleagues and services are fatigued and still dealing with the pressures. This context makes it even more essential that we share the responsibility, learn from each other at least and collaborate with each other at best, and hold each other up to be the best we can.’ (Document U).
Concerns were raised such as the widening of health inequalities since the pandemic and cost of living crisis. Post-pandemic and Brexit, recruiting health, social care and third sector staff was compounding the capacity throughout this already heavily pressurised system.
In [case study], we have seen the stalling of life expectancy and worsening of the health inequality gap, which is expected to be compounded by the effects of the pandemic. (Paraphrased Document T)
‘I think key barriers, just the immense pressure on the system still really […] under a significant workload, catching up on activity, catching up on NHS Health Checks, catching up on long-term condition reviews. There is a significant strain on the system still in terms of catching up. It has been really difficult because of the impact of COVID.’ (LP7).
‘Workforce is a challenge, because the pipelines that we’ve got, we’ve got fewer people coming through many of them. And that’s not just particular to, I don't know, nursing, which is often talking talked [sic] about as a challenged area, isn't it? And of course, it is. But we’ve got similar challenges in social care, in third sector.’ (LP5).
The pandemic was reported to have increased pressures on the NHS and services not only in relation to staff capacity but also regarding increases in referrals to services, such as mental health. Access to healthcare changed during the pandemic increasing barriers for some:
‘I think people are just confused about where they're supposed to go, in terms of accessing health and care at the moment. It's really complex to understand where you're supposed to go, especially, at the moment, coming out of COVID, and the fact that GPs are not the accessible front door. You can't just walk into your GP anymore.’ (LP16).
‘Meeting this increased demand [for work related to reducing ethnic inequalities in mental health] is starting to prove a challenge and necessitates some discussion about future resourcing.’ (Document S)
Several ways were identified to aid effective adaptation and/or mitigation. This included building resilience such as developing the existing capacity, capability and flexibility of the system by learning from previous work, adapting structures and strengthening workforce development. Considerations, such as a commitment to Marmot Principles and how funding could/would contribute, were also discussed.
The funding’s [linked to Core20PLUS5] purpose is to help systems to ensure that health inequalities are not made worse when cost-savings or efficiencies are sought…The available data and insight are clear and [health inequalities are] likely to worsen in the short term, the delays generated by pandemic, the disproportionate effect of that on the most deprived and the worsening food and fuel poverty in all our places. (Paraphrased Document L).
Learning from the pandemic was thought to be useful as some working practices had altered during COVID-19 for the better, such as needing to continue to embed how the system had collaborated and resist old patterns of working:
‘So I think that emphasis between collaboration – extreme collaboration – which is what we did during COVID is great. I suppose the problem is, as we go back into trying to save money, we go back into our old ways of working, about working in silos. And I think we’ve got to be very mindful of that, and continue to work in a different way.’ (LP11).
Another area identified as requiring action, was the collection, analysis, sharing and use of data accessible by the whole system.
‘So I think there is a lot of data out there. It’s just how do we present that in such a way that it’s accessible to everyone as well, because I think sometimes, what happens is that we have one group looking at data in one format, but then how do we cascade that out?’ (LP12)
We aimed to explore a system’s level understanding of how a local area addresses health inequalities with a focus on avoidable emergency admissions using a case study approach. Therefore, the focus of our research was strategic and systematic approaches to inequalities reduction. Gaining an overview of what was occurring within a system is pertinent because local areas are required to have a regard to address health inequalities in their local areas [ 20 , 21 ]. Through this exploration, we also developed an understanding of the system's processes reported to be required. For example, an area requiring action was viewed as the accessibility and analysis of data. The case study described having health inequalities ‘at the heart of its health and wellbeing strategy ’ which was echoed across the documents from multiple sectors across the system. Evidence of a values driven partnership with whole systems working was centred on the importance of place and involving people, with links to a ‘strong third sector ’ . Working together to support and strengthen local assets (the system, services/support, communities/individuals, and the workforce) were vital components. This suggested a system’s committed and integrated approach to improve population health and reduce health inequalities as well as concerted effort to increase system resilience. However, there was juxtaposition at times with what the documents contained versus what interviewees spoke about, for example, the degree to which asset-based approaches were embedded.
Furthermore, despite having a priori codes for the documentary analysis and including specific questions around work being undertaken to reduce health inequalities in avoidable admissions in the interviews with key systems leaders, this explicit link was still very much under-developed for this case study. For example, how to reduce health inequalities in avoidable emergency admissions was not often specified in the documents but could be inferred from existing work. This included work around improving COVID-19 vaccine uptake in groups who were identified as being at high-risk (such as older people and socially excluded populations) by using local intelligence to inform where to offer local outreach targeted pop-up clinics. This limited explicit action linking reduction of health inequalities in avoidable emergency admissions was echoed in the interviews and it became clear as we progressed through the research that a focus on reduction of health inequalities in avoidable hospital admissions at a systems level was not a dominant aspect of people’s work. Health inequalities were viewed as a key part of the work but not necessarily examined together with avoidable admissions. A strengthened will to take action is reported, particularly around reducing health inequalities, but there were limited examples of action to explicitly reduce health inequalities in avoidable admissions. This gap in the systems thinking is important to highlight. When it was explicitly linked, upstream strategies and thinking were acknowledged as requirements to reduce health inequalities in avoidable emergency admissions.
Similar to our findings, other research have also found networks to be considered as the system’s backbone [ 30 ] as well as the recognition that communities need to be central to public health approaches [ 51 , 55 , 56 ]. Furthermore, this study highlighted the importance of understanding the local context by using local routine and bespoke intelligence. It demonstrated that population-based approaches to reduce health inequalities are complex, multi-dimensional and interconnected. It is not about one part of the system but how the whole system interlinks. The interconnectedness and interdependence of the system (and the relevant players/stakeholders) have been reported by other research [ 30 , 57 ], for example without effective exchange of knowledge and information, social networks and systems do not function optimally [ 30 ]. Previous research found that for systems to work effectively, management and transfer of knowledge needs to be collaborative [ 30 ], which was recognised in this case study as requiring action. By understanding the context, including the strengths and challenges, the support or action needed to overcome the barriers can be identified.
There are very limited number of case studies that explore health inequalities with a focus on hospital admissions. Of the existing research, only one part of the health system was considered with interviews looking at data trends [ 35 ]. To our knowledge, this research is the first to build on this evidence by encompassing the wider health system using wider-ranging interviews and documentary analysis. Ford et al. [ 35 ] found that geographical areas typically had plans to reduce total avoidable emergency admissions but not comprehensive plans to reduce health inequalities in avoidable emergency admissions. This approach may indeed widen health inequalities. Health inequalities have considerable health and costs impacts. Pertinently, the hospital care costs associated with socioeconomic inequalities being reported as £4.8 billion a year, mainly due to excess hospitalisations such as avoidable admissions [ 58 ] and the burden of disease lies disproportionately with our most disadvantaged communities, addressing inequalities in hospital pressures is required [ 25 , 26 ].
Implications for research and policy
Improvements to life expectancy have stalled in the UK with a widening of health inequalities [ 12 ]. Health inequalities are not inevitable; it is imperative that the health gap between the deprived and affluent areas is narrowed [ 12 ]. This research demonstrates the complexity and intertwining factors that are perceived to address health inequalities in an area. Despite the evidence of the cost (societal and individual) of avoidable admissions, explicit tackling of inequality in avoidable emergency admissions is not yet embedded into the system, therefore highlights an area for policy and action. This in-depth account and exploration of the characteristics of ‘whole systems’ working to address health inequalities, including where challenges remain, generated in this research will be instrumental for decision makers tasked with addressing health and care inequalities.
This research informs the next step of exploring each identified theme in more detail and moving beyond description to develop tools, using a suite of multidimensional and multidisciplinary methods, to investigate the effects of interventions on systems as previously highlighted by Rutter et al. [ 5 ].
Strengths and limitations
Documentary analysis is often used in health policy research but poorly described [ 44 ]. Furthermore, Yin reports that case study research is often criticised for not adhering to ‘systematic procedures’ p. 18 [ 41 ]. A clear strength of this study was the clearly defined boundary (in time and space) case as well as following a defined systematic approach, with critical thought and rationale provided at each stage [ 34 , 41 ]. A wide range and large number of documents were included as well as interviewees from across the system thereby resulting in a comprehensive case study. Integrating the analysis from two separate methodologies (interviews and documentary analysis), analysed separately before being combined, is also a strength to provide a coherent rich account [ 49 ]. We did not limit the reasons for hospital admission to enable a broad as possible perspective; this is likely to be a strength in this case study as this connection between health inequalities and avoidable hospital admissions was still infrequently made. However, for example, if a specific care pathway for a health condition had been highlighted by key informants this would have been explored.
Due to concerns about identifiability, we took several steps. These included providing a summary of the sectors that the interviewees and document were from but we were not able to specify which sectors each quote pertained. Additionally, some of the document quotes required paraphrasing. However, we followed a set process to ensure this was as rigorous as possible as described in the methods section. For example, where we were required to paraphrase, each paraphrased quote and original was shared and agreed with all the authors to reduce the likelihood to inadvertently misinterpreting or misquoting.
The themes are unlikely to represent an exhaustive list of the key elements requiring attention, but they represent the key themes that were identified using a robust methodological process. The results are from a single urban local authority with high levels of socioeconomic disadvantage in the North of England which may limit generalisability to different contexts. However, the findings are still generalisable to theoretical considerations [ 41 ]. Attempts to integrate a case study with a known framework can result in ‘force-fit’ [ 34 ] which we avoided by developing our own framework (Fig. 1 ) considering other existing models [ 14 , 59 ]. The results are unable to establish causation, strength of association, or direction of influence [ 60 ] and disentangling conclusively what works versus what is thought to work is difficult. The documents’ contents may not represent exactly what occurs in reality, the degree to which plans are implemented or why variation may occur or how variation may affect what is found [ 43 , 61 ]. Further research, such as participatory or non-participatory observation, could address this gap.
Conclusions
This case study provides an in-depth exploration of how local areas are working to address health and care inequalities, with a focus on avoidable hospital admissions. Key elements of this system’s reported approach included fostering strategic coherence, cross-agency working, and community-asset based working. An area requiring action was viewed as the accessibility and analysis of data. Therefore, local areas could consider the challenges of data sharing across organisations as well as the organisational capacity and capability required to generate useful analysis in order to create meaningful insights to assist work to reduce health and care inequalities. This would lead to improved understanding of the context including where the key barriers lie for a local area. Addressing structural barriers and threats as well as supporting the training and wellbeing of the workforce are viewed as key to building resilience within a system to reduce health inequalities. Furthermore, more action is required to embed reducing health inequalities in avoidable admissions explicitly in local areas with inaction risking widening the health gap.
Availability of data and materials
Individual participants’ data that underlie the results reported in this article and a data dictionary defining each field in the set are available to investigators whose proposed use of the data has been approved by an independent review committee for work. Proposals should be directed to [email protected] to gain access, data requestors will need to sign a data access agreement. Such requests are decided on a case by case basis.
Dahlgren G, Whitehead M. Policies and strategies to promote social equity in health. Sweden: Institute for Future Studies Stockholm; 1991.
Google Scholar
Commission on Social Determinants of Health (CSDH). Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health. Geneva: World Health Organisation; 2008.
Marmot M, et al. Fair Society, Healthy Lives (The Marmot Review). London: The Marmot Review; 2010.
Academy of Medical Sciences, Improving the health of the public by 2040: optimising the research environment for a healthier, fairer future. London: The Academy of Medical Sciences; 2016.
Rutter H, et al. The need for a complex systems model of evidence for public health. The Lancet. 2017;390(10112):2602–4.
Article Google Scholar
Diez Roux AV. Complex systems thinking and current impasses in health disparities research. Am J Public Health. 2011;101(9):1627–34.
Article PubMed PubMed Central Google Scholar
Foster-Fishman PG, Nowell B, Yang H. Putting the system back into systems change: a framework for understanding and changing organizational and community systems. Am J Community Psychol. 2007;39(3–4):197–215.
Article PubMed Google Scholar
World Health Organisation (WHO). The World Health Report 2000 health systems: improving performance. Geneva: World Health Organisation; 2000.
Papanicolas I, et al. Health system performance assessment: a framework for policy analysis in Health Policy Series, No. 57. Geneva: World Heath Organisation; 2022.
Bartley M. Health Inequalities: An Introduction to Theories, Concepts and Methods. Cambridge: Polity Press; 2004.
World Health Organization and Finland Ministry of Social Affairs and Health, Health in all policies: Helsinki statement. Framework for country action. Geneva: World Health Organisation; 2014.
Marmot M, et al. Health equity in England: The Marmot Review 10 years on. London: Institute of Health Equity; 2020.
Bambra C, et al. Reducing health inequalities in priority public health conditions: using rapid review to develop proposals for evidence-based policy. J Public Health. 2010;32(4):496–505.
Public Health England, Community-centred public health. Taking a whole system approach. London: Public Health England; 2020.
Davey F, et al. Levelling up health: a practical, evidence-based framework for reducing health inequalities. Public Health in Pract. 2022;4:100322.
Public Health England (PHE). Place-based approaches to reducing health inequalities. PHE; 2021.
Ford J, et al. Transforming health systems to reduce health inequalities. Future Healthc J. 2021;8(2):e204–9.
Olivera JN, et al. Conceptualisation of health inequalities by local healthcare systems: a document analysis. Health Soc Care Community. 2022;30(6):e3977–84.
Department of Health (DoH). Health and Social Care Act 2012. 2012.
Department of Health (DoH). Health and social care act 2022. 2022.
Department of Health (DoH). Statutory guidance on joint strategic needs assessments and joint health and wellbeing strategies. London: Department of Health; 2013.
Asaria M, Doran T, Cookson R. The costs of inequality: whole-population modelling study of lifetime inpatient hospital costs in the English National health service by level of neighbourhood deprivation. J Epidemiol Community Health. 2016;70:990–6.
Castro AC, et al. Local NHS equity trends and their wider determinants: a pilot study of data on emergency admissions. 2020. https://www.york.ac.uk/media/healthsciences/documents/research/Local_NHS_Equity_Trends.pdf .
Nuffield Trust. Potentially preventable emergency admissions. 2023. Available from: https://www.nuffieldtrust.org.uk/resource/potentially-preventable-emergency-hospital-admissions#background .
Cookson R, Asaria M, Ali S, Ferguson B, Fleetcroft R, Goddard M, et al. Health Equity Indicators for the English NHS: a longitudinal whole-population study at the small-area level. Health Serv Deliv Res. 2016;4(26). https://doi.org/10.3310/hsdr04260
Roland M, Abel G. Reducing emergency admissions: are we on the right track? BMJ. 2012;345:e6017.
Moore GF, et al. Process evaluation of complex interventions: medical research council guidance. BMJ. 2015;350:h1258.
Petticrew M. Public health evaluation: epistemological challenges to evidence production and use. Evid Policy. 2013;9:87–95.
Adam T. Advancing the application of systems thinking in health. Health Res Policy Syst. 2014;12(1):1–5.
Leischow SJ, et al. Systems thinking to improve the public’s health. Am J Prev Med. 2008;35:S196–203.
Paparini S, et al. Evaluating complex interventions in context: systematic, meta-narrative review of case study approaches. BMC Med Res Methodo. 2021;21(1):225.
McGill E, et al. Qualitative process evaluation from a complex systems perspective: a systematic review and framework for public health evaluators. PLoS Med. 2020;17(11):e1003368.
Paparini S, et al. Case study research for better evaluations of complex interventions: rationale and challenges. BMC Med. 2020;18(1):301.
Crowe S, et al. The case study approach. BMC Med Res Methodol. 2011;11:100.
Ford J, et al. Reducing inequality in avoidable emergency admissions: case studies of local health care systems in England using a realist approach. Journal of Health Services Research and Policy. 2021;27:27(1).
Stake RE. The art of case study research. Thousand Oaks CA: Sage; 1995.
Ministry of Housing Communities and Local Government and Department for Levelling Up Housing and Communities. English indices of deprivation 2015. 2015. Available from: https://www.gov.uk/government/statistics/english-indices-of-deprivation-2015 .
Whitehead M. Due North: the report of the Inequiry on Health Equity for the North. 2014.
Yin RK. Case study research: design and methods. 5th ed. California: Sage Publications Inc.; 2014.
Castro Avila AC, et al. Local equity data packs for England 2009-2018. 2019. Available from: https://www.york.ac.uk/che/research/equity/monitoring/packs/ .
Yin RK. Case Study Research and Applications: Design and Methods. 6th ed. Los Angeles: SAGE; 2018.
Patton MQ. Qualitative research and evaluation methods. 3rd ed. London: Sage Publications; 2002.
Sowden S, et al. Interventions to reduce inequalities in avoidable hospital admissions: explanatory framework and systematic review protocol. BMJ Open. 2020;10(7):e035429.
Dalglish SL, Kalid H, McMahon SA. Document analysis in health policy research: the READ approach. Health Policy Plan. 2020;35(10):1424–31.
Article PubMed Central Google Scholar
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
Robson C, McCartan K. Real World Research . 4th ed. Chichester, UK: John Wiley & Sons Ltd; 2016.
Bowen GA. Document analysis as a qualitative research method. Qual Res J. 2009;9(2):27–40.
Robson C, McCartan K. Real World Research. 4th ed. Chichester: John Wiley & Sons Ltd; 2016.
Moran-Ellis J, et al. Triangulation and integration: processes, claims and implications. Qual Res. 2006;6(1):45–59.
Parbery-Clark C, et al. Coproduction of a resource sharing public views of health inequalities: an example of inclusive public and patient involvement and engagement. Health Expectations. 2023:27(1):e13860.
Stansfield J, South J, Mapplethorpe T. What are the elements of a whole system approach to community-centred public health? A qualitative study with public health leaders in England’s local authority areas. BMJ Open. 2020;10(8):e036044.
Shams L, Akbari SA, Yazdani S. Values in health policy - a concept analysis. Int J Health Policy Manag. 2016;1(5):623–30.
NHS England. Core20PLUS5 (adults) – an approach to reducing healthcare inequalities. 2021 11/03/2023]. Available from: https://www.england.nhs.uk/about/equality/equality-hub/national-healthcare-inequalities-improvement-programme/core20plus5/ .
Charles A. Integrated care systems explained: making sense of systems, places and neighbourhoods. 2022 24/09/2023]; Available from: https://www.kingsfund.org.uk/publications/integrated-care-systems-explained .
Elwell-Sutton T, et al. Creating healthy lives: a whole-government approach to long-term investment in the nation's health. London: The Health Foundation; 2019.
Buck D, Baylis A, Dougall D. A vision for population health: towards a healthier future. London, UK: The Kings Fund; 2018.
Popay J, et al. System resilience and neighbourhood action on social determinants of health inequalities: an english case study. Perspect Public Health. 2022;142(4):213–23.
Article PubMed PubMed Central CAS Google Scholar
Asaria M, et al. How a universal health system reduces inequalities: lessons from England. J Epidemiol Community Health. 2016;70(7):637–43.
Daniel KD. Introduction to systems thinking. Pegasus Communications, Inc; 1999.
Jessiman PE, et al. A systems map of determinants of child health inequalities in England at the local level. PLoS ONE. 2021;16(2):e0245577.
Sleeman KE, et al. Is end-of-life a priority for policymakers? Qualitative documentary analysis of health care strategies. Palliat Med. 2018;32(9):1464–84.
Download references
Acknowledgements
Thanks to our Understanding Factors that explain Avoidable hospital admission Inequalities - Research study (UNFAIR) PPI contributors, for their involvement in the project particularly in the identification of the key criteria for the sampling frame. Thanks to the research advisory team as well.
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Submission declaration and verification
The manuscript is not currently under consideration or published in another journal. All authors have read and approved the final manuscript.
This research was funded by the National Institute for Health and Care Research (NIHR), grant number (ref CA-CL-2018-04-ST2-010). The funding body was not involved in the study design, collection of data, inter-pretation, write-up, or submission for publication. The views expressed are those of the authors and not necessarily those of the NIHR, the Department of Health and Social Care or Newcastle University.
Author information
Authors and affiliations.
Faculty of Medical Sciences, Public Health Registrar, Population Health Sciences Institute, Newcastle University, Newcastle Upon Tyne, UK
Charlotte Parbery-Clark
Post-Doctoral Research Associate, Faculty of Medical Sciences, Population Health Sciences Institute, Newcastle University, Newcastle Upon Tyne, UK
Lorraine McSweeney
Senior Research Methodologist & Public Involvement Lead, Faculty of Medical Sciences, Population Health Sciences Institute, Newcastle University, Newcastle Upon Tyne, UK
Joanne Lally
Senior Clinical Lecturer &, Faculty of Medical Sciences, Honorary Consultant in Public Health, Population Health Sciences Institute, Newcastle University, Newcastle Upon Tyne, UK
Sarah Sowden
You can also search for this author in PubMed Google Scholar
Contributions
Conceptualization - J.L. and S.S.; methodology - C.P.-C., J.L. & S.S.; formal analysis - C. P.-C. & L.M.; investigation- C. P.-C. & L.M., resources, writing of draft manuscript - C.P.-C.; review and editing manuscript L.M., J.L., & S.S.; visualization including figures and tables - C.P.-C.; supervision - J.L. & S.S.; project administration - L.M. & S.S.; funding acquisition - S.S. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Correspondence to Charlotte Parbery-Clark or Sarah Sowden .
Ethics declarations
Ethics approval and consent to participate.
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Newcastle University (protocol code 13633/2020 on the 12 th of July 2021).
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., supplementary material 2., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Parbery-Clark, C., McSweeney, L., Lally, J. et al. How can health systems approach reducing health inequalities? An in-depth qualitative case study in the UK. BMC Public Health 24 , 2168 (2024). https://doi.org/10.1186/s12889-024-19531-5
Download citation
Received : 20 October 2023
Accepted : 18 July 2024
Published : 10 August 2024
DOI : https://doi.org/10.1186/s12889-024-19531-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Health inequalities
- Complex whole systems approach
- In-depth qualitative case study
BMC Public Health
ISSN: 1471-2458
- General enquiries: [email protected]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
Ambient particulate matter and chronic obstructive pulmonary disease mortality: a nationwide, individual-level, case-crossover study in China
Affiliations.
- 1 School of Public Health, Key Lab of Public Health Safety of the Ministry of Education and NHC Key Lab of Health Technology Assessment, Fudan University, Shanghai, China; Shanghai Pulmonary Hospital, Tongji University School of Medicine, Shanghai, China.
- 2 National Center for Chronic Noncommunicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing, China.
- 3 School of Public Health, Key Lab of Public Health Safety of the Ministry of Education and NHC Key Lab of Health Technology Assessment, Fudan University, Shanghai, China.
- 4 School of Public Health, Key Lab of Public Health Safety of the Ministry of Education and NHC Key Lab of Health Technology Assessment, Fudan University, Shanghai, China. Electronic address: [email protected].
- 5 Department of Respiratory and Critical Care Medicine, Beijing Hospital, National Center of Gerontology; Institute of Geriatric Medicine, Chinese Academy of Medical, Beijing, China. Electronic address: [email protected].
- PMID: 39137570
- DOI: 10.1016/j.ebiom.2024.105270
Background: Short-term exposure to particulate matter air pollution has been associated with the exacerbations of COPD, but its association with COPD mortality was not fully elucidated. We aimed to assess the association between short-term particulate matter exposure and the risk of COPD mortality in China using individual-level data.
Methods: We derived 2.26 million COPD deaths from a national death registry database in Chinese mainland between 2013 and 2019. Exposures to fine particulate matter (PM 2.5 ) and coarse particulate matter (PM 2.5-10 ) were assessed by satellite-based models of a 1 × 1 km resolution and assigned to each individual based on residential address. The associations of PM 2.5 and PM 2.5-10 with COPD mortality were examined using a time-stratified case-crossover design and conditional logistic regressions with distributed lag models. We further conducted stratified analyses by age, sex, education level, and season.
Findings: Short-term exposures to both PM 2.5 and PM 2.5-10 were associated with increased risks of COPD mortality. These associations appeared and peaked on the concurrent day, attenuated and became nonsignificant after 5 or 7 days, respectively. The exposure-response curves were approximately linear without discernible thresholds. An interquartile range increase in PM 2.5 and PM 2.5-10 concentrations was associated with 4.23% (95% CI: 3.75%, 4.72%) and 2.67% (95% CI: 2.18%, 3.16%) higher risks of COPD mortality over lag 0-7 d, respectively. The associations of PM 2.5 and PM 2.5-10 attenuated slightly but were still significant in the mutual-adjustment models. A larger association of PM 2.5-10 was observed in the warm season.
Interpretation: This individual-level, nationwide, case-crossover study suggests that short-term exposure to PM 2.5 and PM 2.5-10 might act as one of the environmental risk factors for COPD mortality.
Funding: This study is supported by the National Key Research and Development Program of China (2023YFC3708304 and 2022YFC3702701), the National Natural Science Foundation of China (82304090 and 82030103), the 3-year Action Plan for Strengthening the Construction of the Public Health System in Shanghai (GWVI-11.2-YQ31), and the Science and Technology Commission of Shanghai Municipality (21TQ015).
Keywords: COPD; Case-crossover study; Coarse particulate matter; Fine particulate matter; Mortality.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
PubMed Disclaimer
Conflict of interest statement
Declaration of interests All authors declare no potential conflicts of interest.
Similar articles
- Mortality and Morbidity Effects of Long-Term Exposure to Low-Level PM 2.5 , BC, NO 2 , and O 3 : An Analysis of European Cohorts in the ELAPSE Project. Brunekreef B, Strak M, Chen J, Andersen ZJ, Atkinson R, Bauwelinck M, Bellander T, Boutron MC, Brandt J, Carey I, Cesaroni G, Forastiere F, Fecht D, Gulliver J, Hertel O, Hoffmann B, de Hoogh K, Houthuijs D, Hvidtfeldt U, Janssen N, Jorgensen J, Katsouyanni K, Ketzel M, Klompmaker J, Hjertager Krog N, Liu S, Ljungman P, Mehta A, Nagel G, Oftedal B, Pershagen G, Peters A, Raaschou-Nielsen O, Renzi M, Rodopoulou S, Samoli E, Schwarze P, Sigsgaard T, Stafoggia M, Vienneau D, Weinmayr G, Wolf K, Hoek G. Brunekreef B, et al. Res Rep Health Eff Inst. 2021 Sep;2021(208):1-127. Res Rep Health Eff Inst. 2021. PMID: 36106702 Free PMC article.
- Mortality-Air Pollution Associations in Low Exposure Environments (MAPLE): Phase 2. Brauer M, Brook JR, Christidis T, Chu Y, Crouse DL, Erickson A, Hystad P, Li C, Martin RV, Meng J, Pappin AJ, Pinault LL, Tjepkema M, van Donkelaar A, Weagle C, Weichenthal S, Burnett RT. Brauer M, et al. Res Rep Health Eff Inst. 2022 Jul;2022(212):1-91. Res Rep Health Eff Inst. 2022. PMID: 36224709 Free PMC article.
- Differential associations of fine and coarse particulate air pollution with cause-specific pneumonia mortality: A nationwide, individual-level, case-crossover study. Zhang Y, He Q, Tong X, Yin P, Liu Y, Meng X, Gao Y, Shi S, Li X, Kan H, Zhou M, Li Y, Chen R. Zhang Y, et al. Environ Res. 2024 Jul 1;252(Pt 3):119054. doi: 10.1016/j.envres.2024.119054. Epub 2024 May 3. Environ Res. 2024. PMID: 38704007
- Assessing Adverse Health Effects of Long-Term Exposure to Low Levels of Ambient Air Pollution: Implementation of Causal Inference Methods. Dominici F, Zanobetti A, Schwartz J, Braun D, Sabath B, Wu X. Dominici F, et al. Res Rep Health Eff Inst. 2022 Jan;2022(211):1-56. Res Rep Health Eff Inst. 2022. PMID: 36193708 Free PMC article. Review.
- Short-term Exposure to Ambient Fine Particulate Matter Increases Hospitalizations and Mortality in COPD: A Systematic Review and Meta-analysis. Li MH, Fan LC, Mao B, Yang JW, Choi AMK, Cao WJ, Xu JF. Li MH, et al. Chest. 2016 Feb;149(2):447-458. doi: 10.1378/chest.15-0513. Epub 2016 Jan 12. Chest. 2016. PMID: 26111257 Review.
- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
Filing an appeal
If you disagree with a coverage or payment decision by Original Medicare , your Medicare Advantage or other Medicare health plan , or your Medicare drug plan you can file an appeal.
Before you start an appeal, ask your provider or supplier for any information that may help your case. If you’re in a Medicare Advantage plan, other health plan, or a drug plan, check your plan materials, or contact your plan, for details about your appeal rights. The plan must tell you, in writing, how to appeal. Generally, you can find your plan's contact information on your plan membership card.
You can file an appeal if Medicare or your plan refuses to:
- Cover a health care service, supply, item, or drug you think Medicare should cover.
- Pay for a health care service, supply, item, or drug you already got.
- Change the amount you must pay for a health care service, supply, item, or drug.
You can also file an appeal if:
- Medicare or your plan stops providing or paying for all or part of a health care service, supply, item, or drug you think you still need.
- Your plan’s drug management program labels you as “at-risk” because you meet the Overutilization Monitoring System criteria. This means your plan limits your access to coverage for drugs like opioids and benzodiazepines.
What if I want to challenge a Local Coverage Determination?
How do appeals work?
The appeals process varies based on the kind of coverage you have. Generally, there are 5 levels of appeals. If you disagree with the decision made at any level of the process, you can usually go to the next level. At each level you'll get a decision letter with instructions on how to move to the next level of appeal.
Get specific information on how to file an appeal based on the kind of coverage you have:
Original Medicare Medicare health plans Medicare drug plans
Can someone help me file an appeal?
State Health Insurance Assistance Program (SHIP): Visit shiphelp.org to get the phone number for your local SHIP and get free, personalized health insurance counseling. SHIPs are state programs that get money from the federal government to give free local health insurance counseling to people with Medicare.
Representative: If you have a trusted family member or friend helping you with a complaint, you can appoint them as a representative. How do I appoint a representative?
Your right to a fast appeal
You also have the right to a fast appeal if you think your Medicare-covered services are ending too soon. This includes services you get from a hospital, skilled nursing facility, home health agency, comprehensive outpatient rehabilitation facility or hospice.
Your provider will give you a written notice before your services end that tells you how to ask for a fast appeal. If they don’t give you this notice, ask for it. Learn more about how fast appeals work.
IMAGES
COMMENTS
An action plan is a detailed roadmap of the necessary steps you need to take to achieve a specific goal or objective. It's like a GPS that guides you from your starting point to your desired destination. Creating an action plan helps you break down a large goal into smaller, more manageable tasks, which makes...
Learn to design effective action plans with our comprehensive guide. Get inspired with examples and ready-to-use templates.
Learn how to write an action plan with steps and tips from Jennifer Bridges, PMP. Watch the video or read the text guide to action plans.
An action plan is a specific list of tasks in order to achieve a particular goal. Learn how to create action plans with templates and examples
Case studies are marketing tools that showcase your customers' success and highlight your brand value. Learn how to write them with examples and templates.
Learn how to write an action plan and improve project management skills. Plus, explore components, action plan examples, formats, and helpful tips.
This guide will show you how to write a case study that engages prospective clients, demonstrates your abilities, and showcases your results.
An action plan is the perfect way to approach goals systematically. We'll cover how to create an action plan and how to implement it successfully.
The Seven Steps of Action Planning. Define the Problem (s) Collect and Analyze the Data. Clarify and Prioritize the Problem (s) Write a Goal Statement for Each Solution. Implement Solutions: The Action Plan. Monitor and Evaluate. Restart with a New Problem, or Refine the Old Problem. The following is a simple example of the problem solving ...
An action plan describes the way your organization will meet its objectives through detailed action steps that describe how and when these steps will be taken. This section provides a guide for developing and utilizing your group's action plan.
Are you struggling with writing your case study's Alternative Courses of Action (ACA)? Here are the steps on how to write one plus a few examples to guide you.
In this Indeed Career Coach approved article, learn how to write an effective action plan and reach your goals more consistently.
Find out what an effective action plan is and how to create one for your project or business. Design your own quickly using our editable action plan templates.
Generally, organize your essay around 1. A definition or position statement (your conclusion) - answers the question what? 2. An argument (your evidence - quantitative and/or qualitative) - answers why? 3. A chronological action plan (steps to solve a problem, implement a decision, improve performance, etc.) - answers how? Writing ...
TOOL 11: SAMPLE CASE STUDIES & ACTION PLANST. S & ACTION PLANS Case Study 1 - Salem Selam is a 17 years old wom. n living in rented accommodation in Beirut. She lives with her moth. r, father, five sisters and three brothers. Salem is unable to spe. k and needs assistance with her daily care. Her mother, Amani, and her two younger sisters ass.
Abstract Qualitative case study methodology enables researchers to conduct an in-depth exploration of intricate phenomena within some specific context. By keeping in mind research students, this article presents a systematic step-by-step guide to conduct a case study in the business discipline. Research students belonging to said discipline face issues in terms of clarity, selection, and ...
The guidance supporting Conservation Action Planning provides you generic how-to information to guide you through the process of completing and iterating a conservation plan.
The plan is a step-by-step guide to drive application on the job. This article describes how this process is used and presents a case study showing how one organization, a large restaurant chain, built evaluation into the performance improvement process and positioned action planning as an application tool.
2 Decisions & Actions Taken Since 1996, in recognition of the above problems and constraints, the Government of Burkina Faso has received technical and financial assistance from the Danish Ministry of Foreign Affairs (Danida). One of the most significant results of this collaboration has been the formulation of the Action Plan for Integrated Water Resources Management in Burkina Faso (PAGIRE ...
The scoping study which informed the action plan identified that the Philippines faces five key challenges in relation to achieving sustainable consumption and production:
Appendix H of the draft Action Plan is not a comprehensive compilation, but includes a select number of water reuse case study summaries that were provided in response to outreach during draft Action Plan development and from the public docket. Along with the abbreviated summaries located in the main body of the draft Action Plan, these ...
Case Study Step #2: Developing a Plan of Action Verification of Understanding Objective: Given the desire to appropriately understand the needs of each student assigned to their care, candidates will develop an action research plan that, if implemented, would begin the process of unpacking the complexity connected to cognitive development. Overview: The Case Study assignments provides evidence ...
The main difference between action research and case study is their purpose; an action research study aims to solve an immediate problem whereas a case study aims to provide an in-depth analysis of a situation or case over a long period of time. 1. What is Action Research?
Action Items. Continue face-to-face marketing effort as capacity for growth allows. Hire new personnel as required by growth demands. Transfer all day-to-day activity management to new managers. Establish Executive Reporting structure and regular meeting agenda. Critical Success Factors: Management Team Development. Succession Plan.
Study design. This in-depth case study is part of an ongoing larger multiple (collective []) case study approach.An instrumental approach [] was taken allowing an in-depth investigation of an issue, event or phenomenon, in its natural real-life context; referred to as a 'naturalistic' design [].Ethics approval was obtained by Newcastle University's Ethics Committee (ref 13633/2020).
This study is supported by the National Key Research and Development Program of China (2023YFC3708304 and 2022YFC3702701), the National Natural Science Foundation of China (82304090 and 82030103), the 3-year Action Plan for Strengthening the Construction of the Public Health System in Shanghai (GWVI …
The plan must tell you, in writing, how to appeal. Generally, you can find your plan's contact information on your plan membership card. You can file an appeal if Medicare or your plan refuses to: Cover a health care service, supply, item, or drug you think Medicare should cover. Pay for a health care service, supply, item, or drug you already got.